

Long-term results after aortic valve replacement for bicuspid or tricuspid valve morphology in a Swedish population
- PMID: 33179723
- PMCID: PMC8043765
- DOI: 10.1093/ejcts/ezaa348
Long-term results after aortic valve replacement for bicuspid or tricuspid valve morphology in a Swedish population
Abstract
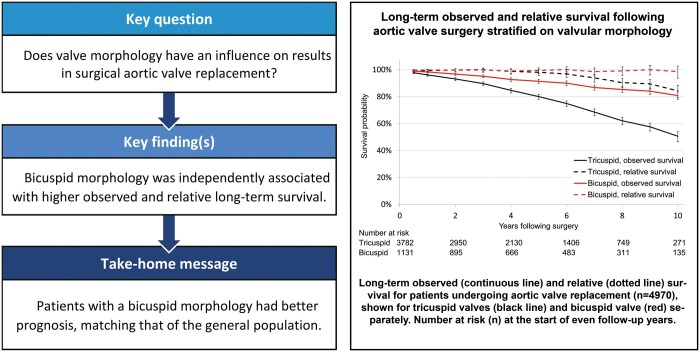
Objectives: Our goal was to study long-term observed and relative survival after first-time aortic valve replacement surgery with or without concomitant coronary artery bypass surgery with reference to valve morphology (i.e. bicuspid vs tricuspid).
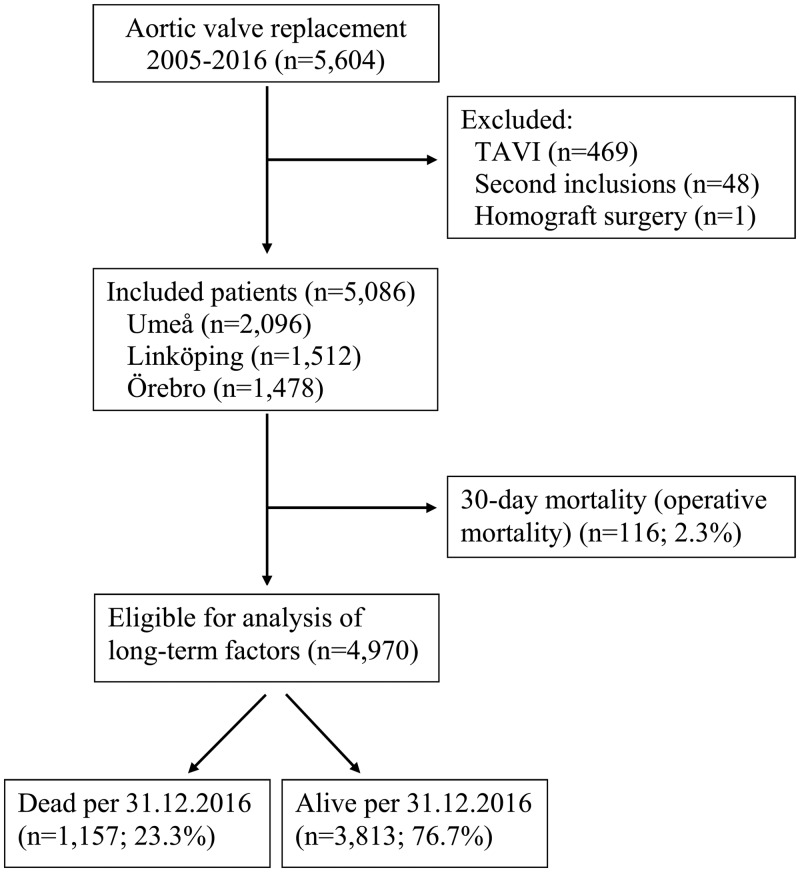
Methods: Consecutive patients (n = 5086) from 3 Swedish hospitals, operated on between 1 January 2005 and 31 December 2016, were included. The 30-day mortality (n = 116, 2.3%) was excluded from the analysis of long-term observed and relative survival (n = 4970). Observed survival was analysed using Cox regression. Relative survival was calculated as the ratio between observed and expected survival based on data from the general Swedish population, matched for age, sex and calendar year. Risk factors for death were explored using multivariable analysis.
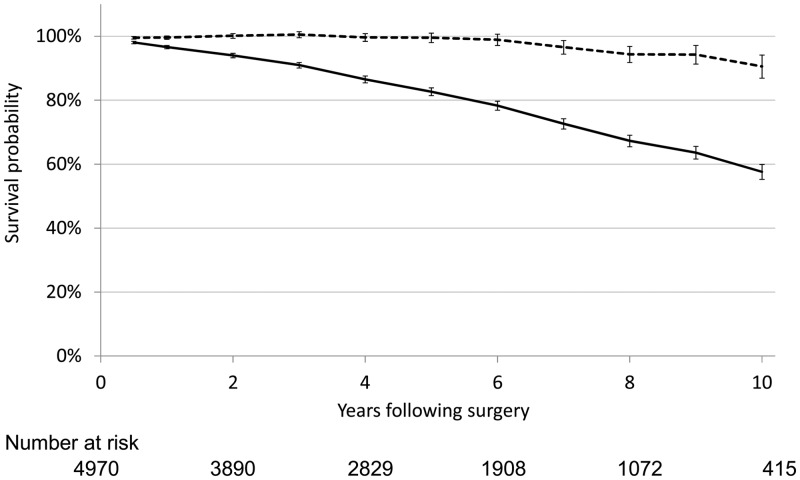
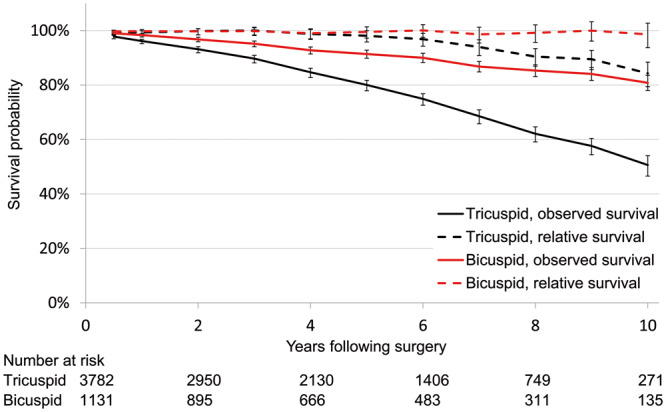
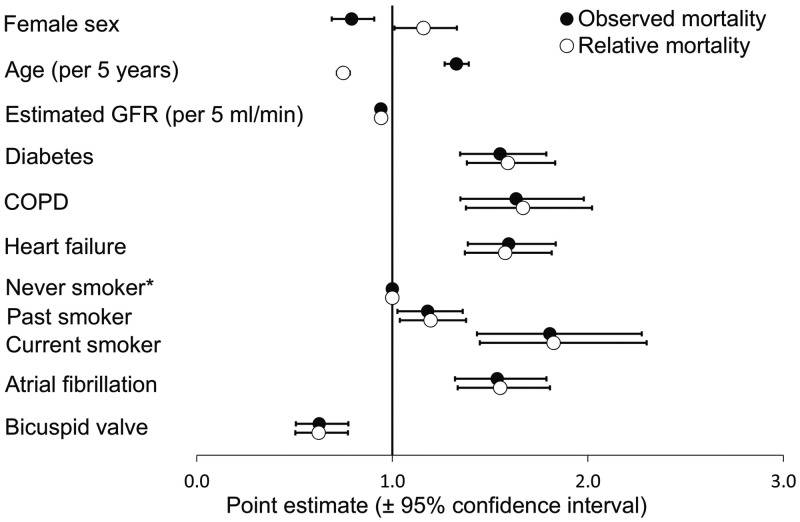
Results: During the follow-up (median 4.7 years) period, 1157 (23%) patients died. Observed survival excluding 30-day mortality was 96.6%, 82.7% and 57.6% after 1, 5 and 10 years. Compared with the general Swedish population, the relative 1-, 5- and 10-year survival rates were 99.0%, 97.5% and 89.0%. Bicuspid morphology was independently associated with higher observed and relative long-term survival. Renal dysfunction, diabetes, chronic obstructive pulmonary disease, heart failure, smoking and atrial fibrillation were associated with higher long-term mortality. Combined surgery was not associated with higher observed or relative mortality.
Conclusions: Patients with a bicuspid morphology had better prognosis, matching that of the general population. With increased age, long-term relative survival compared favourably with survival in the general Swedish population. Adding coronary artery bypass surgery to an aortic valve replacement procedure did not affect long-term outcome.
Keywords: Aortic stenosis; Aortic valve replacement; Bicuspid valve; Observed survival; Relative survival.
© The Author(s) 2020. Published by Oxford University Press on behalf of the European Association for Cardio-Thoracic Surgery.
Figures
References
-
- Yoon SH, Bleiziffer S, De Backer O, Delgado V, Arai T, Ziegelmueller J. et al. Outcomes in transcatheter aortic valve replacement for bicuspid versus tricuspid aortic valve stenosis. J Am Coll Cardiol 2017;69:2579–89. - PubMed
-
- Gao D, Grunwald GK, Rumsfeld JS, Schooley L, MacKenzie T, Shroyer AL.. Time-varying risk factors for long-term mortality after coronary artery bypass graft surgery. Ann Thorac Surg 2006;81:793–9. - PubMed
-
- Statistics Sweden: Life Table by Sex and Age. Year 1960–2018 (Data Obtained through the Human Mortality Database). www.mortality.org (16 February 2018, date last accessed).
-
- Dickman PW, Coviello E.. Estimating and modeling relative survival. Stata J 2015;15:186–215.
