

Dose Reduction of Preoperative Radiotherapy in Myxoid Liposarcoma: A Nonrandomized Controlled Trial
- PMID: 33180100
- PMCID: PMC7662477
- DOI: 10.1001/jamaoncol.2020.5865
Dose Reduction of Preoperative Radiotherapy in Myxoid Liposarcoma: A Nonrandomized Controlled Trial
Abstract
Importance: Currently, preoperative radiotherapy for all soft-tissue sarcomas is identical at a 50-Gy dose level, which can be associated with morbidity, particularly wound complications. The observed clinical radiosensitivity of the myxoid liposarcoma subtype might offer the possibility to reduce morbidity.
Objective: To assess whether a dose reduction of preoperative radiotherapy for myxoid liposarcoma would result in comparable oncological outcome with less morbidity.
Design, setting, and participants: The Dose Reduction of Preoperative Radiotherapy in Myxoid Liposarcomas (DOREMY) trial is a prospective, single-group, phase 2 nonrandomized controlled trial being conducted in 9 tertiary sarcoma centers in Europe and the US. Participants include adults with nonmetastatic, biopsy-proven and translocation-confirmed myxoid liposarcoma of the extremity or trunk who were enrolled between November 24, 2010, and August 1, 2019. Data analyses, using both per-protocol and intention-to-treat approaches, were conducted from November 24, 2010, to January 31, 2020.
Interventions: The experimental preoperative radiotherapy regimen consisted of 36 Gy in once-daily 2-Gy fractions, with subsequent definitive surgical resection after an interval of 4 or more weeks.
Main outcomes and measures: As a short-term evaluable surrogate for local control, the primary end point was centrally reviewed pathologic treatment response. The experimental regimen was regarded as a success when 70% or more of the resection specimens showed extensive treatment response, defined as 50% or greater of the tumor volume containing treatment effects. Morbidity outcomes consisted of wound complications and late toxic effects.
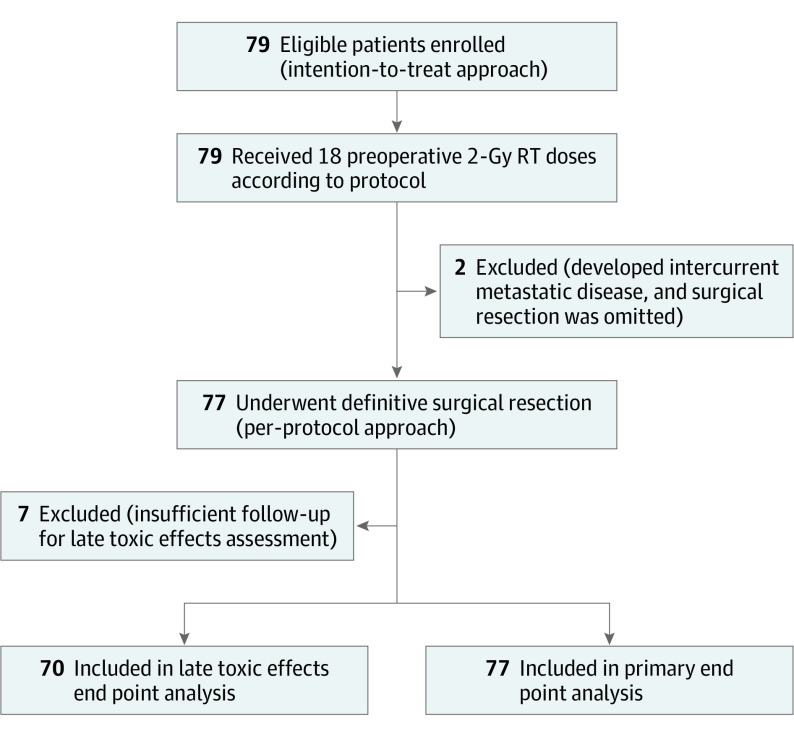
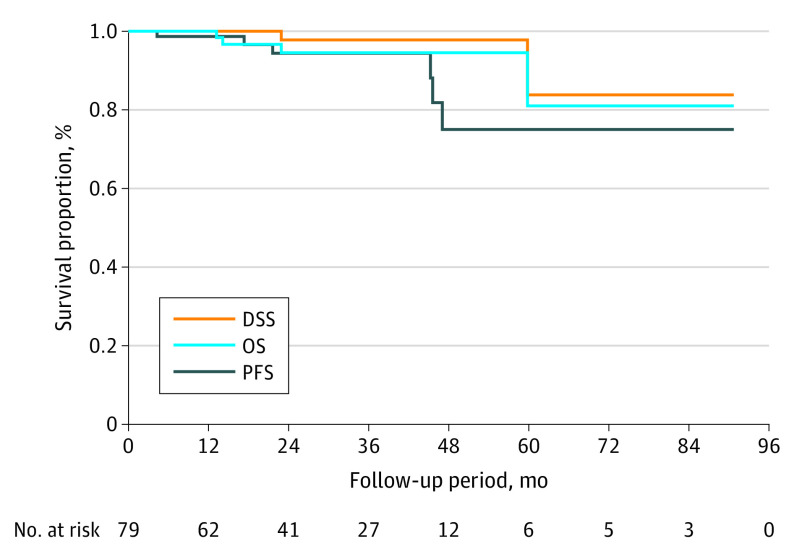
Results: Among the 79 eligible patients, 44 (56%) were men and the median (interquartile range) age was 45 (39-56) years. Two patients did not undergo surgical resection because of intercurrent metastatic disease. Extensive pathological treatment response was observed in 70 of 77 patients (91%; posterior mean, 90.4%; 95% highest probability density interval, 83.8%-96.4%). The local control rate was 100%. The rate of wound complication requiring intervention was 17%, and the rate of grade 2 or higher toxic effects was 14%.
Conclusions and relevance: The findings of the DOREMY nonrandomized clinical trial suggest that deintensification of preoperative radiotherapy dose is effective and oncologically safe and is associated with less morbidity than historical controls, although differences in radiotherapy techniques and follow-up should be considered. A 36-Gy dose delivered in once-daily 2-Gy fractions is proposed as a dose-fractionation approach for myxoid liposarcoma, given that phase 3 trials are logistically impossible to execute in rare cancers.
Trial registration: ClinicalTrials.gov Identifier: NCT02106312.
Conflict of interest statement
Figures
References
-
- Antonescu CR, Ladanyi M. Myxoid liposarcoma In: Fletcher CDM, Bridge JA, Hogendoorn PCW, Mertens F, eds. WHO Classification of Tumours of Soft Tissue and Bone. International Agency for Research on Cancer; 2013:39-41.
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
