

Trends, Perioperative Adverse Events, and Survival of Patients With Left Ventricular Assist Devices Undergoing Noncardiac Surgery
- PMID: 33180131
- PMCID: PMC7662145
- DOI: 10.1001/jamanetworkopen.2020.25118
Trends, Perioperative Adverse Events, and Survival of Patients With Left Ventricular Assist Devices Undergoing Noncardiac Surgery
Abstract
Importance: Information regarding the performance and outcomes of noncardiac surgery (NCS) in patients with left ventricular assist devices (LVADs) is scarce, with limited longitudinal follow-up data that are mostly limited to single-center reports.
Objective: To examine the trends, patient characteristics, and outcomes associated with NCS among patients with LVAD.
Design, setting, and participants: This cohort study examined patients enrolled in Medicare undergoing durable LVAD implantation from January 2012 to November 2017 with follow-up through December 2017. The study included all Medicare Provider and Analysis Review Part A files for the years 2012 to 2017. Patients identified by International Classification of Diseases, Ninth Revision Clinical Modification (ICD-9-CM) and International Classification of Diseases, Tenth Revision (ICD-10) procedure codes for new LVAD implantation were included. Data analysis was performed from November 2019 to February 2020.
Exposures: NCS procedures were identified using the ICD-9-CM and ICD-10 procedural codes and divided into elective and urgent or emergent.
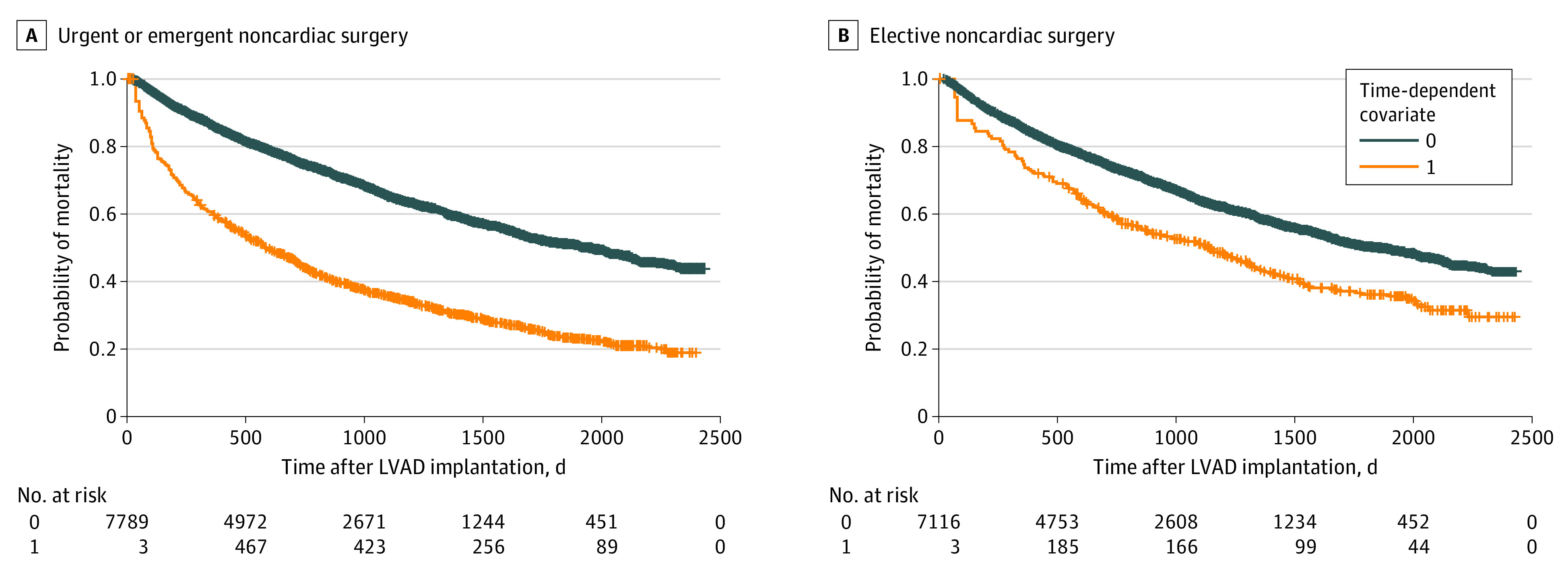
Main outcomes and measures: The primary outcome was major adverse cardiovascular events (MACEs), defined as in-hospital or 30-day all-cause mortality, ischemic stroke, or intracerebral hemorrhage after NCS. Early (<60 days after NCS) and late (≥60 days after NCS) mortality after NCS were analyzed in both subgroups using time-varying covariate and landmark analysis using patients who did not undergo NCS as reference.
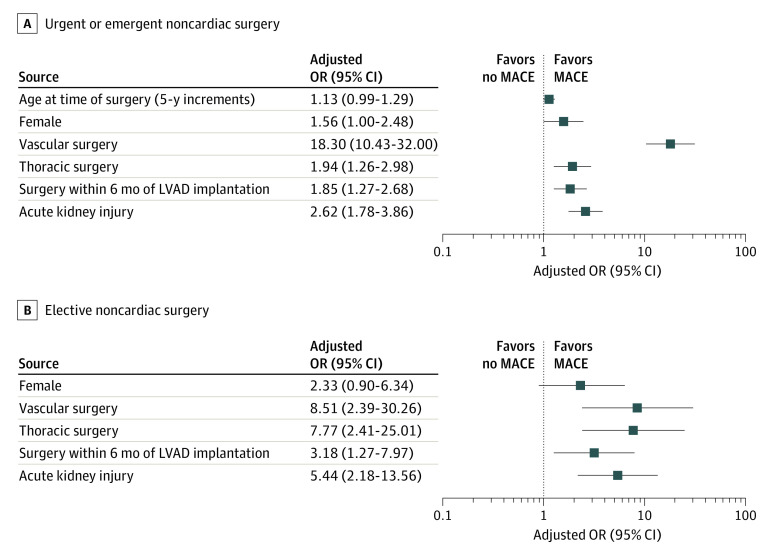
Results: Of the 8118 patients with LVAD (mean [SD] age, 63.4 [10.8] years; 6484 men [79.9%]), 1326 (16.3%, or approximately 1 in 6) underwent NCS, of which 1000 procedures (75.4%) were emergent or urgent and 326 (24.6%) were elective. There was no difference in age between patients who underwent NCS and patients who did not (mean [SD] age, 63.6 [10.6] vs 63.4 [10.9] years). The number of NCS procedures among patients with LVAD increased from 64 in 2012 to 304 in 2017. The median (interquartile range) time from LVAD implantation to NCS was 309 (133-606) days. The most frequent type of NCS was general (613 abdominal, pelvic, and gastrointestinal procedures [46.2%]). Perioperative MACEs occurred in 169 patients (16.9%) undergoing emergent or urgent NCS and 23 patients (7.1%) undergoing elective NCS. Urgent or emergent NCS was associated with higher mortality early (adjusted hazard ratio [aHR], 8.78; 95% CI, 7.20-10.72; P < .001) and late (aHR, 1.71; 95% CI, 1.53-1.90; P < .001) after NCS compared with patients with LVAD who did not undergo NCS. Elective NCS was also associated with higher mortality early (aHR, 2.65; 95% CI, 1.74-4.03; P < .001) and late (aHR, 1.29; 95% CI, 1.07-1.56; P = .008) after NCS.
Conclusions and relevance: One of 6 patients with LVAD underwent NCS. Perioperative MACEs were frequent. Higher mortality risk transcended the early postoperative period in urgent or emergent and elective surgical procedures.
Conflict of interest statement
Figures
Comment in
-
Translating Outcomes Data Into Improved Shared Decision-Making in Patients With Left Ventricular Assist Devices.JAMA Netw Open. 2020 Nov 2;3(11):e2025673. doi: 10.1001/jamanetworkopen.2020.25673. JAMA Netw Open. 2020. PMID: 33180126 No abstract available.
References
-
- Yancy CW, Jessup M, Bozkurt B, et al. . 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;128(16):e240-e327. doi:10.1161/CIR.0b013e31829e8776 - DOI - PubMed
-
- Ponikowski P, Voors AA, Anker SD, et al. ; ESC Scientific Document Group . 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC), developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2016;37(27):2129-2200. doi:10.1093/eurheartj/ehw128 - DOI - PubMed
-
- Rose EA, Gelijns AC, Moskowitz AJ, et al. ; Randomized Evaluation of Mechanical Assistance for the Treatment of Congestive Heart Failure (REMATCH) Study Group . Long-term use of a left ventricular assist device for end-stage heart failure. N Engl J Med. 2001;345(20):1435-1443. doi:10.1056/NEJMoa012175 - DOI - PubMed
