

Bidirectional associations between COVID-19 and psychiatric disorder: retrospective cohort studies of 62 354 COVID-19 cases in the USA
- PMID: 33181098
- PMCID: PMC7820108
- DOI: 10.1016/S2215-0366(20)30462-4
Bidirectional associations between COVID-19 and psychiatric disorder: retrospective cohort studies of 62 354 COVID-19 cases in the USA
Erratum in
-
Correction to Lancet Psychiatry 2020; published online Nov 9. https://doi.org/10.1016/S2215-0366(20)30462-4.Lancet Psychiatry. 2021 Jan;8(1):e1. doi: 10.1016/S2215-0366(20)30509-5. Epub 2020 Nov 12. Lancet Psychiatry. 2021. PMID: 33189218 Free PMC article. No abstract available.
Abstract
Background: Adverse mental health consequences of COVID-19, including anxiety and depression, have been widely predicted but not yet accurately measured. There are a range of physical health risk factors for COVID-19, but it is not known if there are also psychiatric risk factors. In this electronic health record network cohort study using data from 69 million individuals, 62 354 of whom had a diagnosis of COVID-19, we assessed whether a diagnosis of COVID-19 (compared with other health events) was associated with increased rates of subsequent psychiatric diagnoses, and whether patients with a history of psychiatric illness are at a higher risk of being diagnosed with COVID-19.
Methods: We used the TriNetX Analytics Network, a global federated network that captures anonymised data from electronic health records in 54 health-care organisations in the USA, totalling 69·8 million patients. TriNetX included 62 354 patients diagnosed with COVID-19 between Jan 20, and Aug 1, 2020. We created cohorts of patients who had been diagnosed with COVID-19 or a range of other health events. We used propensity score matching to control for confounding by risk factors for COVID-19 and for severity of illness. We measured the incidence of and hazard ratios (HRs) for psychiatric disorders, dementia, and insomnia, during the first 14 to 90 days after a diagnosis of COVID-19.
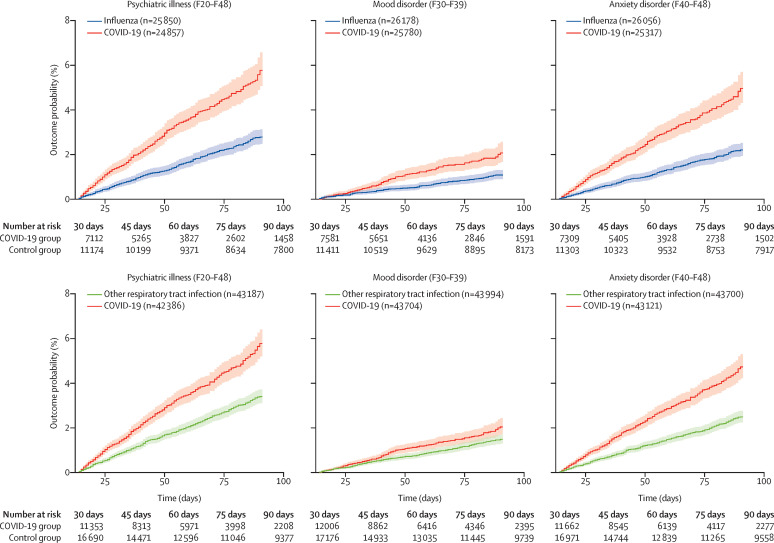
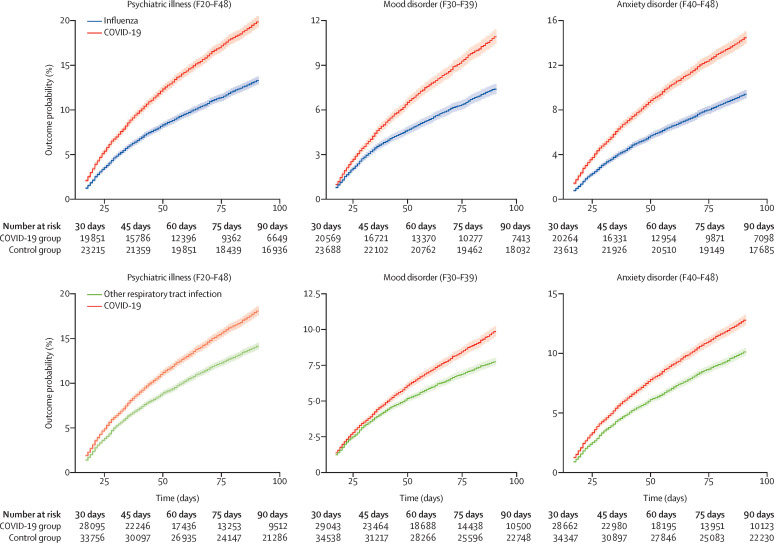
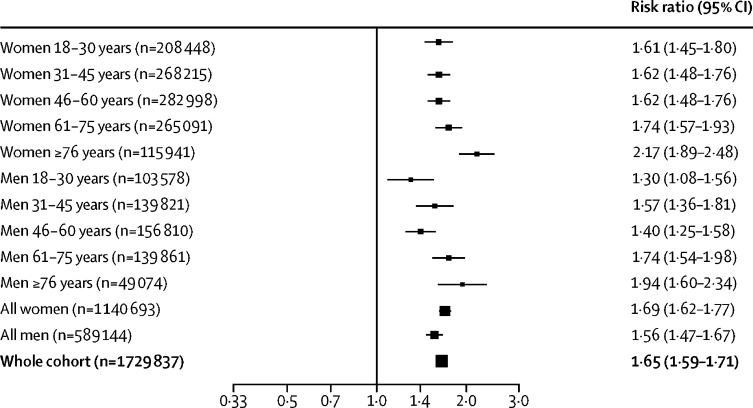
Findings: In patients with no previous psychiatric history, a diagnosis of COVID-19 was associated with increased incidence of a first psychiatric diagnosis in the following 14 to 90 days compared with six other health events (HR 2·1, 95% CI 1·8-2·5 vs influenza; 1·7, 1·5-1·9 vs other respiratory tract infections; 1·6, 1·4-1·9 vs skin infection; 1·6, 1·3-1·9 vs cholelithiasis; 2·2, 1·9-2·6 vs urolithiasis, and 2·1, 1·9-2·5 vs fracture of a large bone; all p<0·0001). The HR was greatest for anxiety disorders, insomnia, and dementia. We observed similar findings, although with smaller HRs, when relapses and new diagnoses were measured. The incidence of any psychiatric diagnosis in the 14 to 90 days after COVID-19 diagnosis was 18·1% (95% CI 17·6-18·6), including 5·8% (5·2-6·4) that were a first diagnosis. The incidence of a first diagnosis of dementia in the 14 to 90 days after COVID-19 diagnosis was 1·6% (95% CI 1·2-2·1) in people older than 65 years. A psychiatric diagnosis in the previous year was associated with a higher incidence of COVID-19 diagnosis (relative risk 1·65, 95% CI 1·59-1·71; p<0·0001). This risk was independent of known physical health risk factors for COVID-19, but we cannot exclude possible residual confounding by socioeconomic factors.
Interpretation: Survivors of COVID-19 appear to be at increased risk of psychiatric sequelae, and a psychiatric diagnosis might be an independent risk factor for COVID-19. Although preliminary, our findings have implications for clinical services, and prospective cohort studies are warranted.
Funding: National Institute for Health Research.
Copyright © 2021 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Disentangling the complex bidirectional associations between COVID-19 and psychiatric disorder.Lancet Psychiatry. 2021 Mar;8(3):179. doi: 10.1016/S2215-0366(20)30565-4. Lancet Psychiatry. 2021. PMID: 33610218 Free PMC article. No abstract available.
-
Disentangling the complex bidirectional associations between COVID-19 and psychiatric disorder - Authors' reply.Lancet Psychiatry. 2021 Mar;8(3):179. doi: 10.1016/S2215-0366(21)00028-6. Lancet Psychiatry. 2021. PMID: 33610219 Free PMC article. No abstract available.
-
Differential follow-up patterns in COVID-19 and comparison cohorts.Lancet Psychiatry. 2021 May;8(5):360. doi: 10.1016/S2215-0366(21)00066-3. Epub 2021 Mar 10. Lancet Psychiatry. 2021. PMID: 33713621 Free PMC article. No abstract available.
-
Differential follow-up patterns in COVID-19 and comparison cohorts - Authors' reply.Lancet Psychiatry. 2021 May;8(5):360-361. doi: 10.1016/S2215-0366(21)00076-6. Epub 2021 Mar 10. Lancet Psychiatry. 2021. PMID: 33713624 Free PMC article. No abstract available.
References
-
- WHO Mental health and psychosocial considerations during the COVID-19 outbreak. March 18, 2020. https://www.who.int/docs/default-source/coronaviruse/mental-health-consi...
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
