

Characteristics and outcomes of neonatal SARS-CoV-2 infection in the UK: a prospective national cohort study using active surveillance
- PMID: 33181124
- PMCID: PMC7818530
- DOI: 10.1016/S2352-4642(20)30342-4
Characteristics and outcomes of neonatal SARS-CoV-2 infection in the UK: a prospective national cohort study using active surveillance
Abstract
Background: Babies differ from older children with regard to their exposure to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). However, data describing the effect of SARS-CoV-2 in this group are scarce, and guidance is variable. We aimed to describe the incidence, characteristics, transmission, and outcomes of SARS-CoV-2 infection in neonates who received inpatient hospital care in the UK.
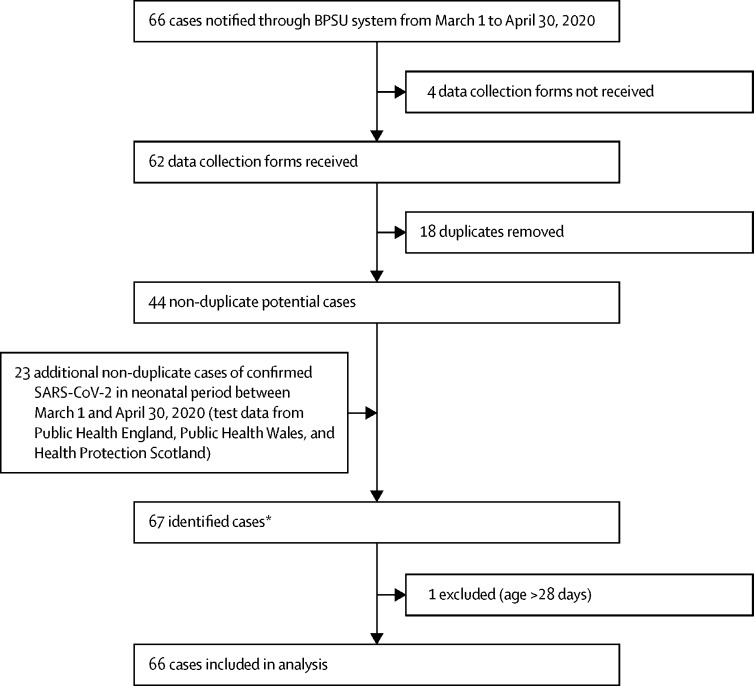
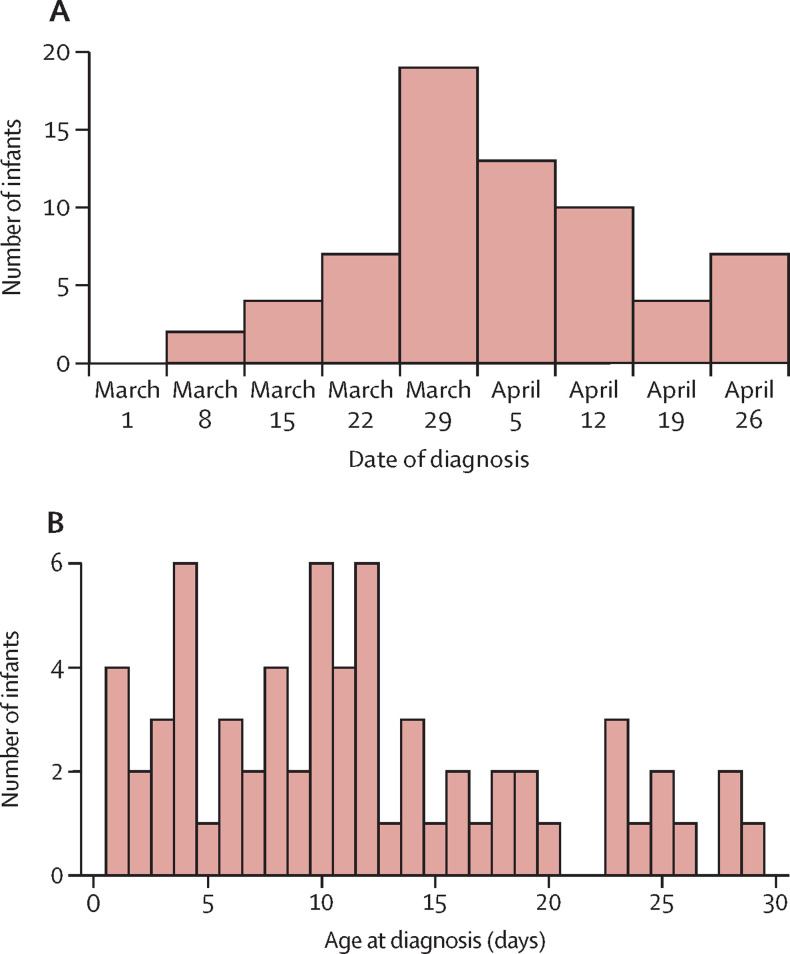
Methods: We carried out a prospective UK population-based cohort study of babies with confirmed SARS-CoV-2 infection in the first 28 days of life who received inpatient care between March 1 and April 30, 2020. Infected babies were identified through active national surveillance via the British Paediatric Surveillance Unit, with linkage to national testing, paediatric intensive care audit, and obstetric surveillance data. Outcomes included incidence (per 10 000 livebirths) of confirmed SARS-CoV-2 infection and severe disease, proportions of babies with suspected vertically and nosocomially acquired infection, and clinical outcomes.
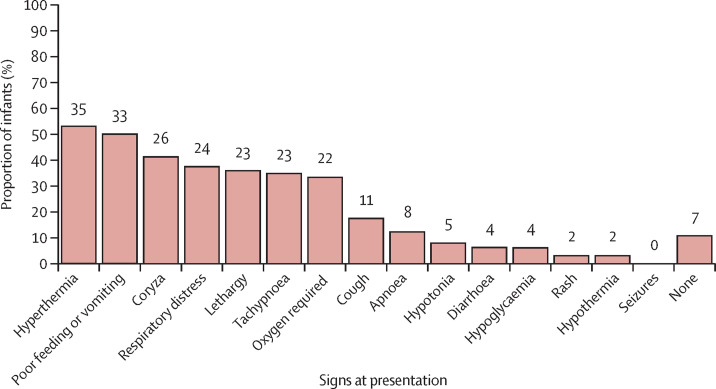
Findings: We identified 66 babies with confirmed SARS-CoV-2 infection (incidence 5·6 [95% CI 4·3-7·1] per 10 000 livebirths), of whom 28 (42%) had severe neonatal SARS-CoV-2 infection (incidence 2·4 [1·6-3·4] per 10 000 livebirths). 16 (24%) of these babies were born preterm. 36 (55%) babies were from white ethnic groups (SARS-CoV-2 infection incidence 4·6 [3·2-6·4] per 10 000 livebirths), 14 (21%) were from Asian ethnic groups (15·2 [8·3-25·5] per 10 000 livebirths), eight (12%) were from Black ethnic groups (18·0 [7·8-35·5] per 10 000 livebirths), and seven (11%) were from mixed or other ethnic groups (5·6 [2·2-11·5] per 10 000 livebirths). 17 (26%) babies with confirmed infection were born to mothers with known perinatal SARS-CoV-2 infection, two (3%) were considered to have possible vertically acquired infection (SARS-CoV-2-positive sample within 12 h of birth where the mother was also positive). Eight (12%) babies had suspected nosocomially acquired infection. As of July 28, 2020, 58 (88%) babies had been discharged home, seven (11%) were still admitted, and one (2%) had died of a cause unrelated to SARS-CoV-2 infection.
Interpretation: Neonatal SARS-CoV-2 infection is uncommon in babies admitted to hospital. Infection with neonatal admission following birth to a mother with perinatal SARS-CoV-2 infection was unlikely, and possible vertical transmission rare, supporting international guidance to avoid separation of mother and baby. The high proportion of babies from Black, Asian, or minority ethnic groups requires investigation.
Funding: UK National Institute for Health Research Policy Research Programme.
Copyright © 2021 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
The ability of the neonatal immune response to handle SARS-CoV-2 infection - Authors' reply.Lancet Child Adolesc Health. 2021 Mar;5(3):e8. doi: 10.1016/S2352-4642(21)00004-3. Epub 2021 Jan 21. Lancet Child Adolesc Health. 2021. PMID: 33484657 Free PMC article. No abstract available.
-
The ability of the neonatal immune response to handle SARS-CoV-2 infection.Lancet Child Adolesc Health. 2021 Mar;5(3):e6-e7. doi: 10.1016/S2352-4642(21)00002-X. Epub 2021 Jan 21. Lancet Child Adolesc Health. 2021. PMID: 33484660 Free PMC article. No abstract available.
-
Unravelling the epidemiology and clinical impact of SARS-CoV-2 infection in neonates.Acta Paediatr. 2021 Aug;110(8):2482-2483. doi: 10.1111/apa.15899. Epub 2021 May 29. Acta Paediatr. 2021. PMID: 34053113 Free PMC article. No abstract available.
References
-
- Dong Y, Mo X, Hu Y, et al. Epidemiology of COVID-19 among children in China. Pediatrics. 2020;145 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
