

Bougie-assisted endotracheal intubation in the pragmatic airway resuscitation trial
- PMID: 33181232
- PMCID: PMC7855993
- DOI: 10.1016/j.resuscitation.2020.11.003
Bougie-assisted endotracheal intubation in the pragmatic airway resuscitation trial
Abstract
Objective: Paramedics may perform endotracheal intubation (ETI) while treating patients with out-of-hospital cardiac arrest (OHCA). The gum elastic Bougie (Bougie) is an intubation adjunct that may optimize intubation success. There are few reports of Bougie-assisted intubation in OHCA nor its association with outcomes. We compared intubation success rates and OHCA outcomes between Bougie-assisted and non-Bougie ETI in the out-of-hospital Pragmatic Airway Resuscitation Trial (PART).
Methods: This was a secondary analysis of patients receiving ETI enrolled in the Pragmatic Airway Resuscitation Trial (PART), a multicenter clinical trial comparing intubation-first vs. laryngeal tube-first strategies of airway management in adult OHCA. The primary exposure was use of Bougie for ETI-assistance. The primary endpoint was first-pass ETI success. Secondary endpoints included overall ETI success, time to successful ETI, return of spontaneous circulation, 72-h survival, hospital survival and hospital survival with favorable neurologic status (Modified Rankin Score ≤3). We analyzed the data using Generalized Estimating Equations and Cox Regression, adjusting for known confounders.
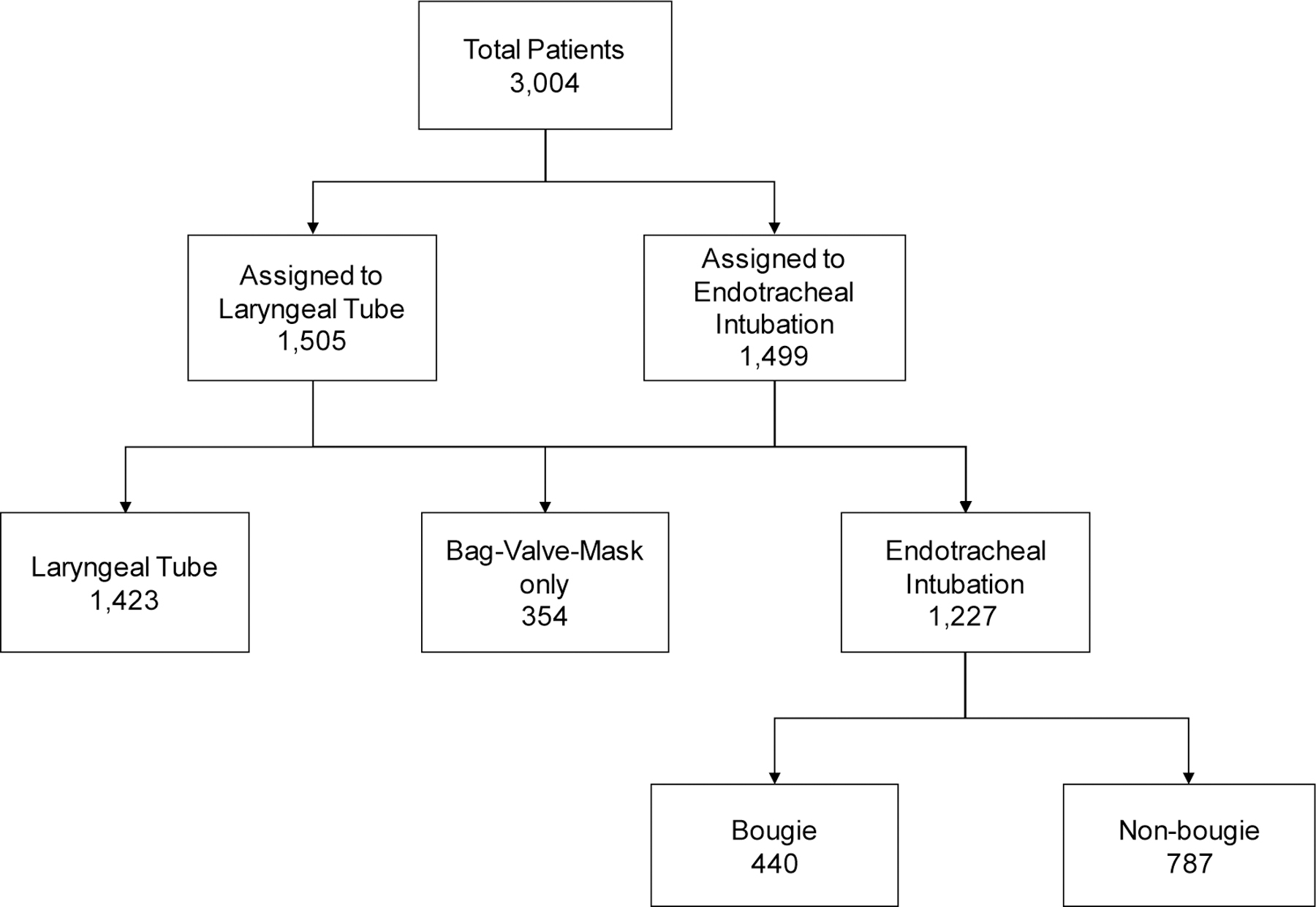
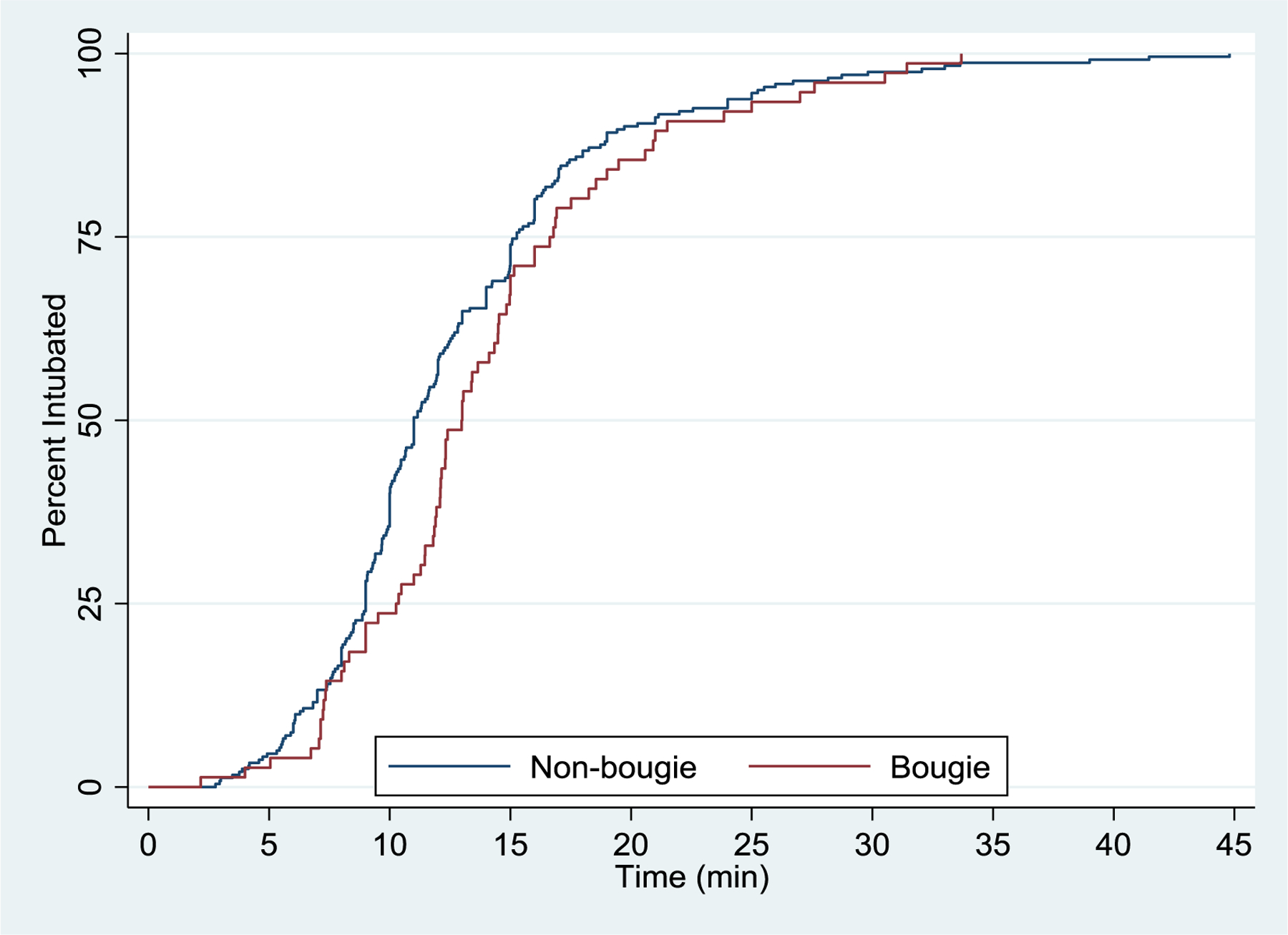
Results: Of the 3004 patients enrolled in PART, 1227 received ETI, including 440 (35.9%) Bougie-assisted and 787 (64.1%) non-Bougie ETIs. First-pass ETI success did not differ between Bougie-assisted and non-Bougie ETI (53.1% vs. 42.8%; adjusted OR 1.12, 95% CI: 0.97-1.39). ETI overall success was slightly higher in the Bougie-assisted group (56.2% vs. 49.1%; adjusted OR 1.19, 95% CI: 1.01-1.32). Time to endotracheal tube placement or abandonment was longer for Bougie-assisted than non-Bougie ETI (median 13 vs. 11 min; adjusted HR 0.63, 95% CI: 0.45-0.90). While survival to hospital discharge was lower for Bougie-assisted than non-Bougie ETI (3.6% vs. 7.5%; adjusted OR 0.94, 95% CI: 0.92-0.96), there were no differences in ROSC, 72-h survival or hospital survival or hospital survival with favorable neurologic status.
Conclusion: While exhibiting slightly higher ETI overall success rates, Bougie-assisted ETI entailed longer airway placement times and potentially lower survival. The role of the Bougie assistance in ETI of OHCA remains unclear.
Keywords: Airway management; Cardiopulmonary arrest; Emergency medical service; Intubation.
Copyright © 2020 Elsevier B.V. All rights reserved.
Figures
References
-
- Hasegawa K, Shigemitsu K, Hagiwara Y, et al. Association between repeated intubation attempts and adverse events in emergency departments: an analysis of a multicenter prospective observational study. Annals of emergency medicine. 2012;60:749–754 e742. - PubMed
-
- Wang HE, Mann NC, Mears G, Jacobson K, Yealy DM. Out-of-hospital airway management in the United States. Resuscitation. 2011;82:378–385. - PubMed
-
- Nwanne T, Jarvis J, Barton D, Donnelly JP, Wang HE. Advanced airway management success rates in a national cohort of emergency medical services agencies. Resuscitation. 2020;146:43–49. - PubMed
-
- Wang HE, Kupas DF, Paris PM, Bates RR, Costantino JP, Yealy DM. Multivariate predictors of failed prehospital endotracheal intubation. Academic emergency medicine : official journal of the Society for Academic Emergency Medicine. 2003;10:717–724. - PubMed
-
- Wang HE, Kupas DF, Paris PM, Bates RR, Yealy DM. Preliminary experience with a prospective, multi-centered evaluation of out-of-hospital endotracheal intubation. Resuscitation. 2003;58:49–58. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
