

Associations of Late Adolescent or Young Adult Cardiovascular Health With Premature Cardiovascular Disease and Mortality
- PMID: 33181243
- PMCID: PMC8100998
- DOI: 10.1016/j.jacc.2020.10.002
Associations of Late Adolescent or Young Adult Cardiovascular Health With Premature Cardiovascular Disease and Mortality
Abstract
Background: When measured in adolescence or young adulthood, cardiovascular health (CVH) is associated with future subclinical cardiovascular disease (CVD), but data are lacking regarding CVD events or mortality.
Objectives: This study examined associations of CVH at ages 18 to 30 years with premature CVD and mortality.
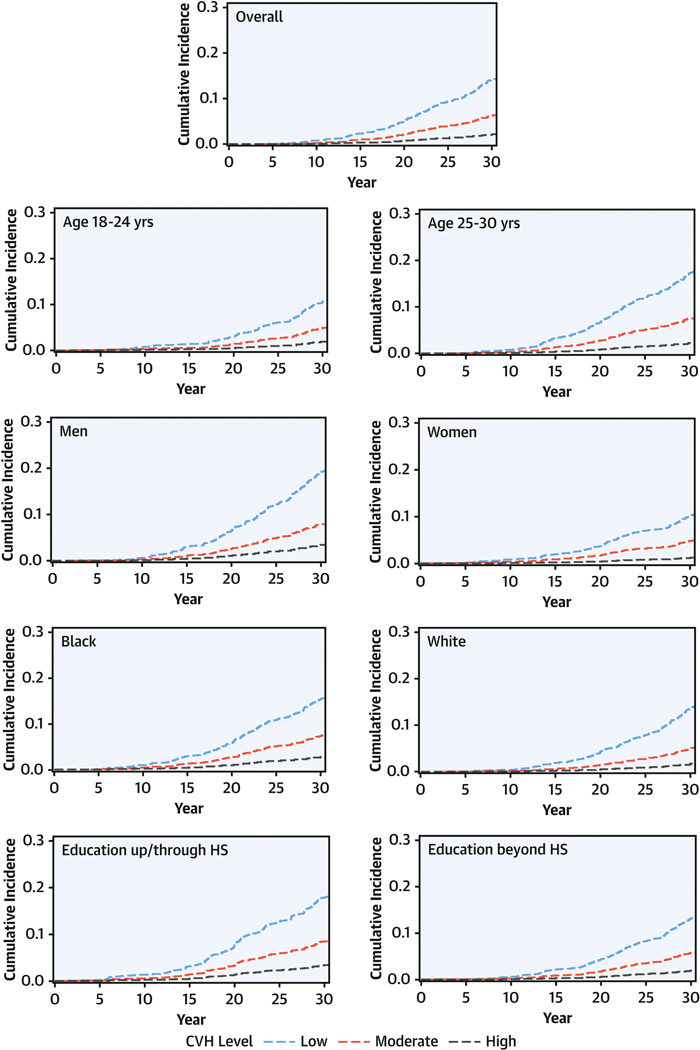
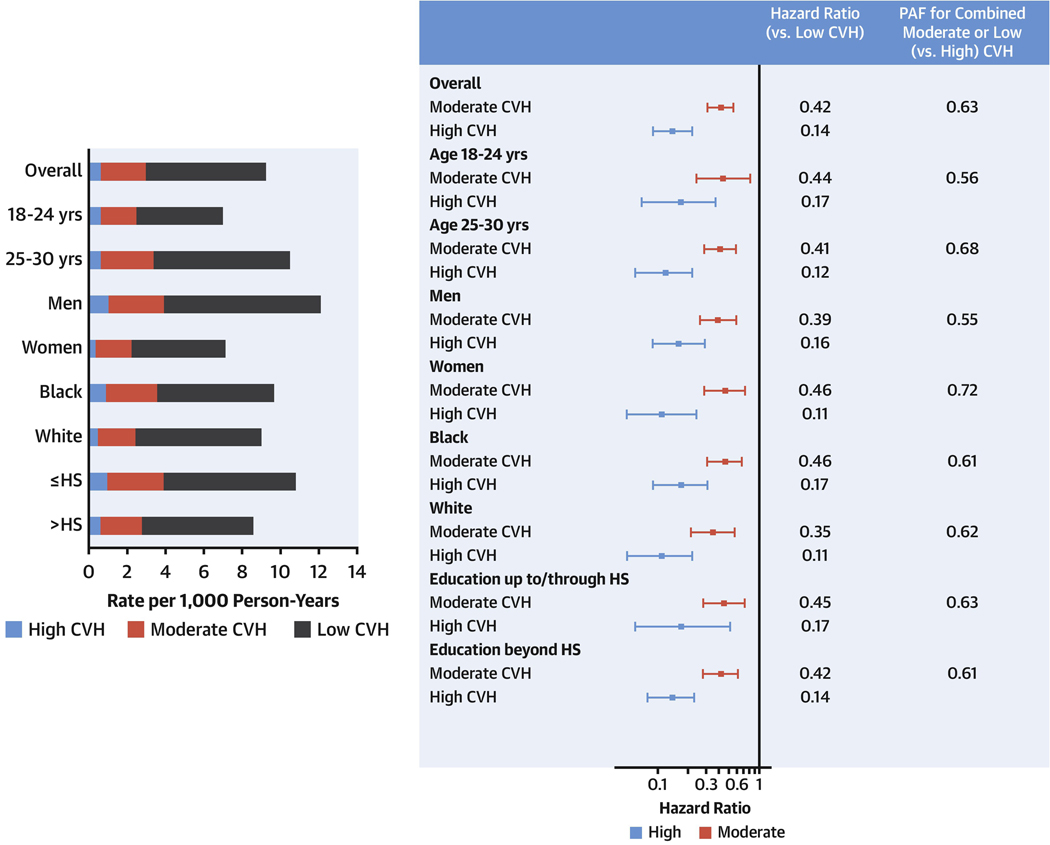
Methods: This study analyzed data from the CARDIA (Coronary Artery Risk Development in Young Adults Study). CVH was scored at baseline (1985 to 1986) using Life's Simple 7 metrics and categorized as high (12 to 14 points), moderate (8 to 11), or low (0 to 7). CVD events and cause-specific mortality were adjudicated over 32 years of follow-up. Adjusted associations were estimated using Cox models and event rates and population attributable fractions were calculated by CVH category.
Results: Among 4,836 participants (mean age: 24.9 years, 54.8% female, 50.5% Black, mean education: 15.2 years), baseline CVH was high (favorable) in 28.8%, moderate in 65.0%, and low in 6.3%. During follow-up, 306 CVD events and 431 deaths occurred. The adjusted hazard ratios for high (vs. low) CVH were 0.14 (95% confidence interval [CI]: 0.09 to 0.22) for CVD and 0.07 (95% CI: 0.03 to 0.19) for CVD mortality, and the population attributable fractions for combined moderate or low (vs. high) CVH were 0.63 (95% CI: 0.47 to 0.74) for CVD and 0.81 (95% CI: 0.55 to 0.92) for CVD mortality. Among individuals with high CVH, event rates were low across sociodemographic subgroups (e.g., CVD rates per 1,000 person-years: age 18 to 24 years, 0.64; age 25 to 30 years, 0.65; men, 1.04; women, 0.36; Blacks, 0.90; Whites, 0.50; up to/through high-school education, 1.00; beyond high-school education, 0.61).
Conclusions: High CVH in late adolescence or young adulthood was associated with very low rates of premature CVD and mortality over 32 years, indicating the critical importance of maintaining high CVH.
Keywords: Life’s Simple 7; population attributable fraction; primordial prevention.
Copyright © 2020 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Author Disclosures The CARDIA study is conducted and supported by the National Heart, Lung, and Blood Institute (NHLBI) in collaboration with the University of Alabama at Birmingham (HHSN268201800005I and HHSN268201800007I), Northwestern University (HHSN268201800003I), University of Minnesota (HHSN268201800006I), Kaiser Foundation Research Institute (HHSN268201800004I), and the Johns Hopkins University School of Medicine (HHSN268200900041C). Dr. Perak has received support from Career Development Award K23 HL145101 from the NHLBI. Dr. Khan has received support from awards from the National Institutes of Health/NHLBI and National Center for Advancing Translational Sciences (KL2TR001424) and the American Heart Association (19TPA34890060). All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures


Comment in
-
Life Course Developmental Approach to Cardiovascular Health and Cardiovascular Disease Prevention: Opportunities and Unanswered Questions.J Am Coll Cardiol. 2020 Dec 8;76(23):2708-2711. doi: 10.1016/j.jacc.2020.10.011. J Am Coll Cardiol. 2020. PMID: 33272364 Free PMC article. No abstract available.
References
-
- Lloyd-Jones DM, Hong Y, Labarthe D et al. Defining and setting national goals for cardiovascular health promotion and disease reduction. Circulation 2010;121:586–613. - PubMed
-
- Virani SS, Alonso A, Benjamin EJ et al. Heart Disease and Stroke Statistics-2020 Update. Circulation 2020;141:e139-e596. - PubMed
-
- Laitinen TT, Pahkala K, Magnussen CG et al. Ideal cardiovascular health in childhood and cardiometabolic outcomes in adulthood. Circulation 2012;125:1971–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
