

Prevalence and Outcomes of Concomitant Aortic Stenosis and Cardiac Amyloidosis
- PMID: 33181246
- PMCID: PMC7805267
- DOI: 10.1016/j.jacc.2020.11.006
Prevalence and Outcomes of Concomitant Aortic Stenosis and Cardiac Amyloidosis
Abstract
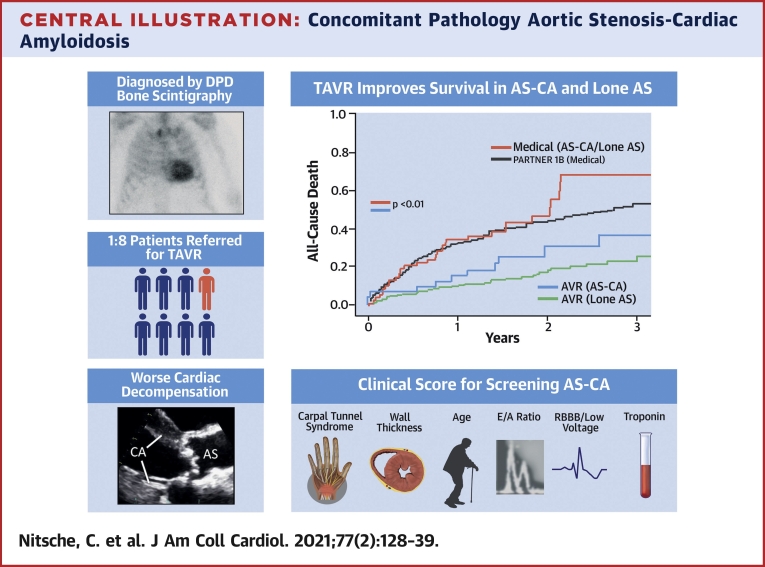
Background: Older patients with severe aortic stenosis (AS) are increasingly identified as having cardiac amyloidosis (CA). It is unknown whether concomitant AS-CA has worse outcomes or results in futility of transcatheter aortic valve replacement (TAVR).
Objectives: This study identified clinical characteristics and outcomes of AS-CA compared with lone AS.
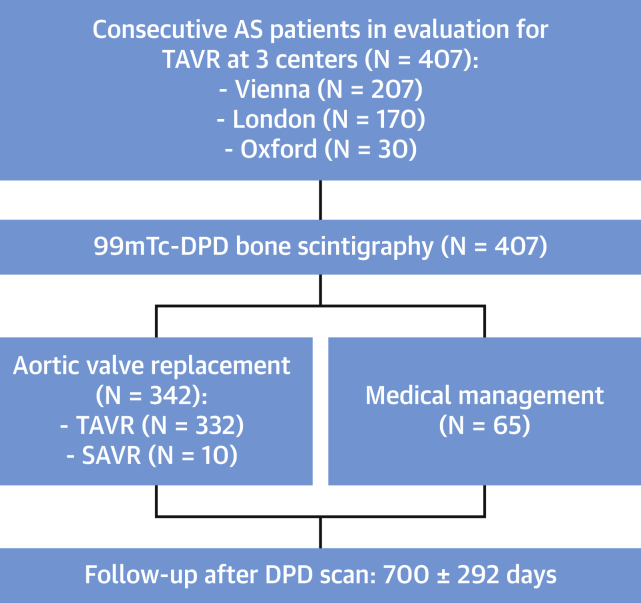
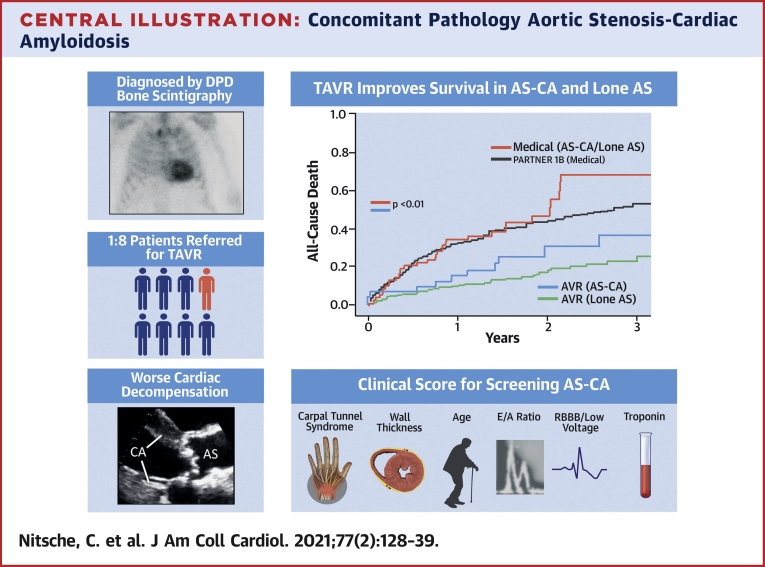
Methods: Patients who were referred for TAVR at 3 international sites underwent blinded research core laboratory 99mtechnetium-3,3-diphosphono-1,2-propanodicarboxylic acid (DPD) bone scintigraphy (Perugini grade 0: negative; grades 1 to 3: increasingly positive) before intervention. Transthyretin-CA (ATTR) was diagnosed by DPD and absence of a clonal immunoglobulin, and light-chain CA (AL) was diagnosed via tissue biopsy. National registries captured all-cause mortality.
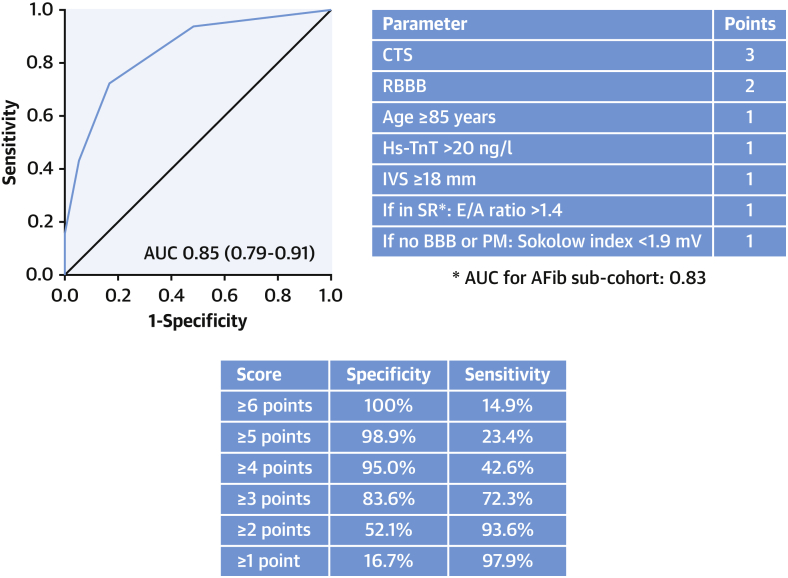
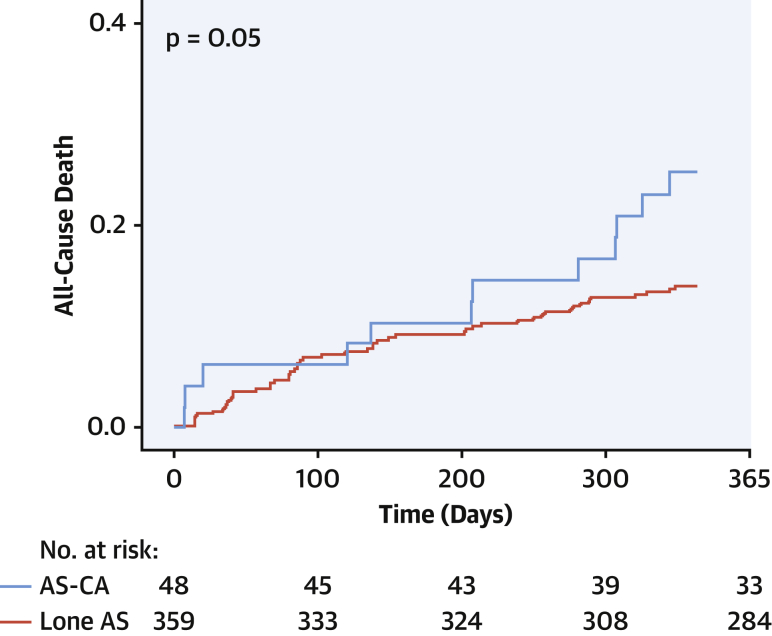
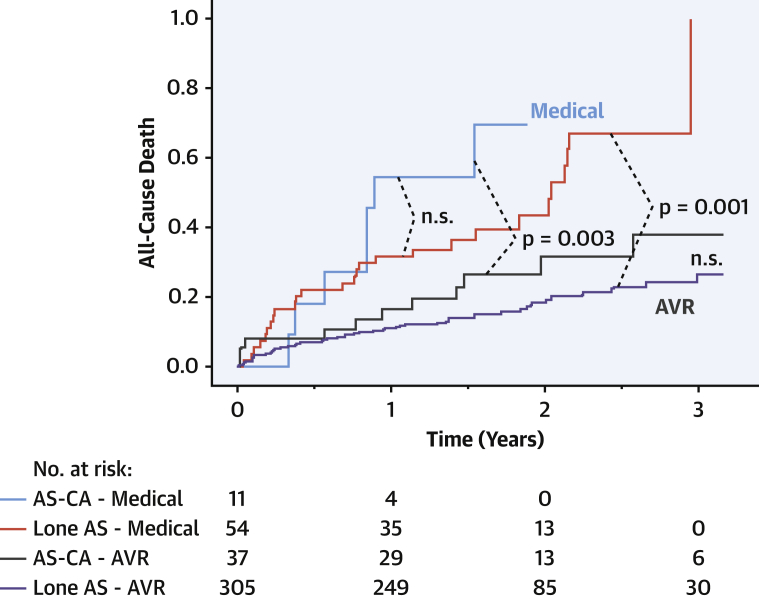
Results: A total of 407 patients (age 83.4 ± 6.5 years; 49.8% men) were recruited. DPD was positive in 48 patients (11.8%; grade 1: 3.9% [n = 16]; grade 2/3: 7.9% [n = 32]). AL was diagnosed in 1 patient with grade 1. Patients with grade 2/3 had worse functional capacity, biomarkers (N-terminal pro-brain natriuretic peptide and/or high-sensitivity troponin T), and biventricular remodeling. A clinical score (RAISE) that used left ventricular remodeling (hypertrophy/diastolic dysfunction), age, injury (high-sensitivity troponin T), systemic involvement, and electrical abnormalities (right bundle branch block/low voltages) was developed to predict the presence of AS-CA (area under the curve: 0.86; 95% confidence interval: 0.78 to 0.94; p < 0.001). Decisions by the heart team (DPD-blinded) resulted in TAVR (333 [81.6%]), surgical AVR (10 [2.5%]), or medical management (65 [15.9%]). After a median of 1.7 years, 23% of patients died. One-year mortality was worse in all patients with AS-CA (grade: 1 to 3) than those with lone AS (24.5% vs. 13.9%; p = 0.05). TAVR improved survival versus medical management; AS-CA survival post-TAVR did not differ from lone AS (p = 0.36).
Conclusions: Concomitant pathology of AS-CA is common in older patients with AS and can be predicted clinically. AS-CA has worse clinical presentation and a trend toward worse prognosis, unless treated. Therefore, TAVR should not be withheld in AS-CA.
Keywords: TAVR; aortic stenosis; cardiac amyloidosis.
Copyright © 2021 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Author Disclosures The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Comment in
-
Concomitant Cardiac Amyloidosis in Severe Aortic Stenosis: The Trojan Horse?J Am Coll Cardiol. 2021 Jan 19;77(2):140-143. doi: 10.1016/j.jacc.2020.11.007. Epub 2020 Nov 9. J Am Coll Cardiol. 2021. PMID: 33181245 No abstract available.
References
-
- Coffey S., Cox B., Williams M.J. The prevalence, incidence, progression, and risks of aortic valve sclerosis: a systematic review and meta-analysis. J Am Coll Cardiol. 2014;63:2852–2861. - PubMed
-
- Schwarz F., Baumann P., Manthey J. The effect of aortic valve replacement on survival. Circulation. 1982;66:1105–1110. - PubMed
-
- Gertz M.A., Dispenzieri A., Sher T. Pathophysiology and treatment of cardiac amyloidosis. Nat Rev Cardiol. 2015;12:91–102. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
