

A Novel 3-Dimensional Printing Fabrication Approach for the Production of Pediatric Airway Models
- PMID: 33181556
- PMCID: PMC8505162
- DOI: 10.1213/ANE.0000000000005260
A Novel 3-Dimensional Printing Fabrication Approach for the Production of Pediatric Airway Models
Abstract
Background: Pediatric airway models currently available for use in education or simulation do not replicate anatomy or tissue responses to procedures. Emphasis on mass production with sturdy but homogeneous materials and low-fidelity casting techniques diminishes these models' abilities to realistically represent the unique characteristics of the pediatric airway, particularly in the infant and younger age ranges. Newer fabrication technologies, including 3-dimensional (3D) printing and castable tissue-like silicones, open new approaches to the simulation of pediatric airways with greater anatomical fidelity and utility for procedure training.
Methods: After ethics approval, available/archived computerized tomography data sets of patients under the age of 2 years were reviewed to identify those suitable for designing new models. A single 21-month-old subject was selected for 3D reconstruction. Manual thresholding was then performed to produce 3D models of selected regions and tissue types within the dataset, which were either directly 3D-printed or later cast in 3D-printed molds with a variety of tissue-like silicones. A series of testing mannequins derived using this multimodal approach were then further refined following direct clinician feedback to develop a series of pediatric airway model prototypes.
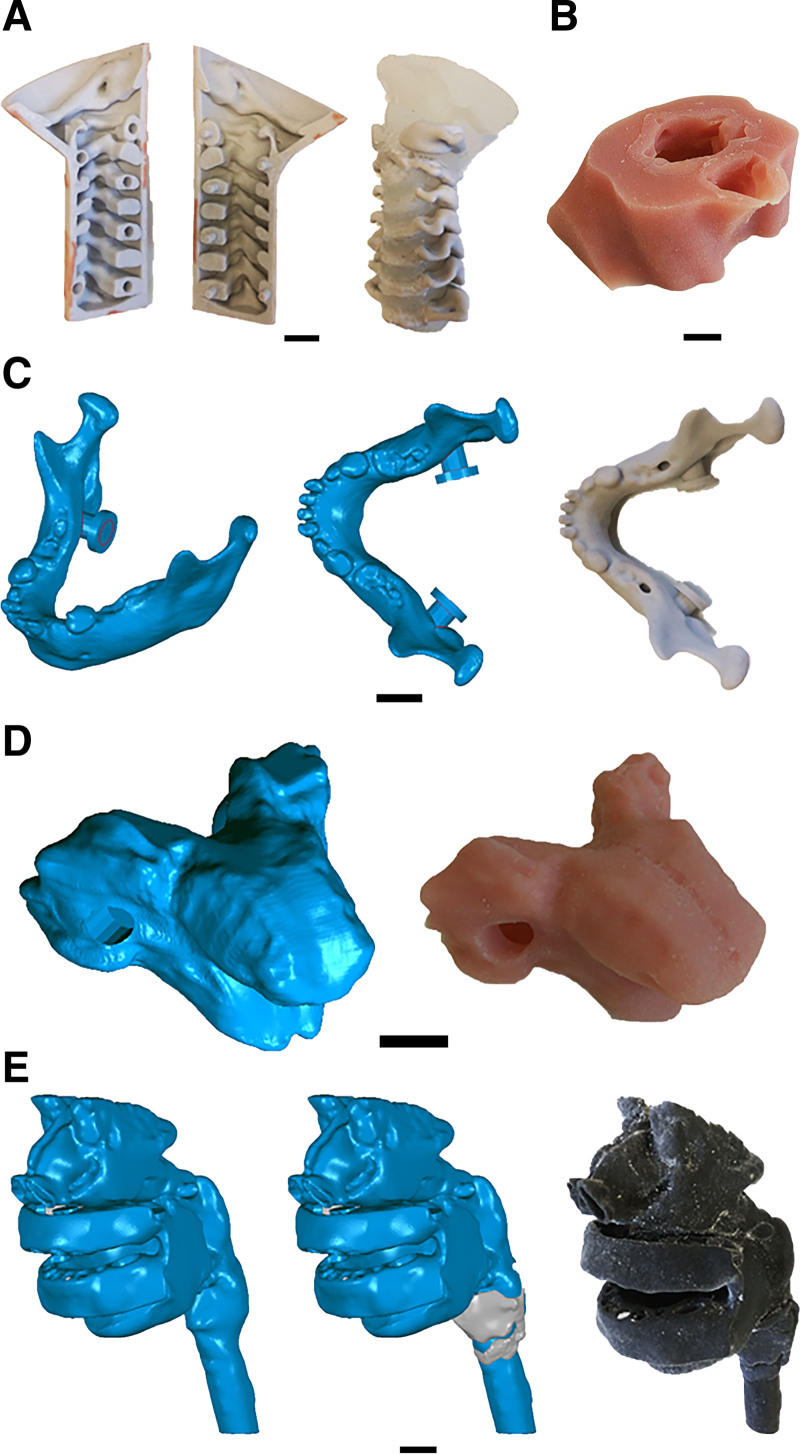
Results: The initial prototype consisted of separate skeletal (skull, mandible, vertebrae) and soft-tissue (nasal mucosa, pharynx, larynx, gingivae, tongue, functional temporomandibular joint [TMJ] "sleeve," skin) modules. The first iterations of these modules were generated using both single-material and multimaterial 3D printing techniques to achieve the haptic properties of real human tissues. After direct clinical feedback, subsequent prototypes relied on a combination of 3D printing for osseous elements and casting of soft-tissue components from 3D-printed molds, which refined the haptic properties of the nasal, oropharyngeal, laryngeal, and airway tissues, and improved the range of movement required for airway management procedures. This approach of modification based on clinical feedback resulted in superior functional performance.
Conclusions: Our hybrid manufacturing approach, merging 3D-printed components and 3D-printed molds for silicone casting, allows a more accurate representation of both the anatomy and functional characteristics of the pediatric airway for model production. Further, it allows for the direct translation of anatomy derived from real patient medical imaging into a functional airway management simulator, and our modular design allows for modification of individual elements to easily vary anatomical configurations, haptic qualities of components or exchange components to replicate pathology.
Copyright © 2020 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the International Anesthesia Research Society.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures


References
-
- Fiadjoe JE, Nishisaki A, Jagannathan N, et al. Airway management complications in children with difficult tracheal intubation from the pediatric difficult intubation (PeDI) registry: a prospective cohort analysis. Lancet Respir Med. 2016;4:37–48. - PubMed
-
- Heinrich S, Birkholz T, Ihmsen H, Irouschek A, Ackermann A, Schmidt J. Incidence and predictors of difficult laryngoscopy in 11,219 pediatric anesthesia procedures. Paediatr Anaesth. 2012;22:729–736. - PubMed
-
- Belanger J, Kossick M. Methods of identifying and managing the difficult airway in the pediatric population. AANA J. 2015;83:35–41. - PubMed
-
- Engelhardt T, Virag K, Veyckemans F, Habre W; APRICOT Group of the European Society of Anaesthesiology Clinical Trial Network. Airway management in paediatric anaesthesia in Europe-insights from APRICOT (anaesthesia practice in children observational trial): a prospective multicentre observational study in 261 hospitals in Europe. Br J Anaesth. 2018;121:66–75. - PubMed
-
- Cook TM, Woodall N, Frerk C; Fourth National Audit Project. Major complications of airway management in the UK: results of the fourth National audit project of the Royal College of Anaesthetists and the difficult airway society. Part 1: anaesthesia. Br J Anaesth. 2011;106:617–631. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
