

Leigh Syndrome Due to NDUFV1 Mutations Initially Presenting as LBSL
- PMID: 33182419
- PMCID: PMC7697158
- DOI: 10.3390/genes11111325
Leigh Syndrome Due to NDUFV1 Mutations Initially Presenting as LBSL
Abstract
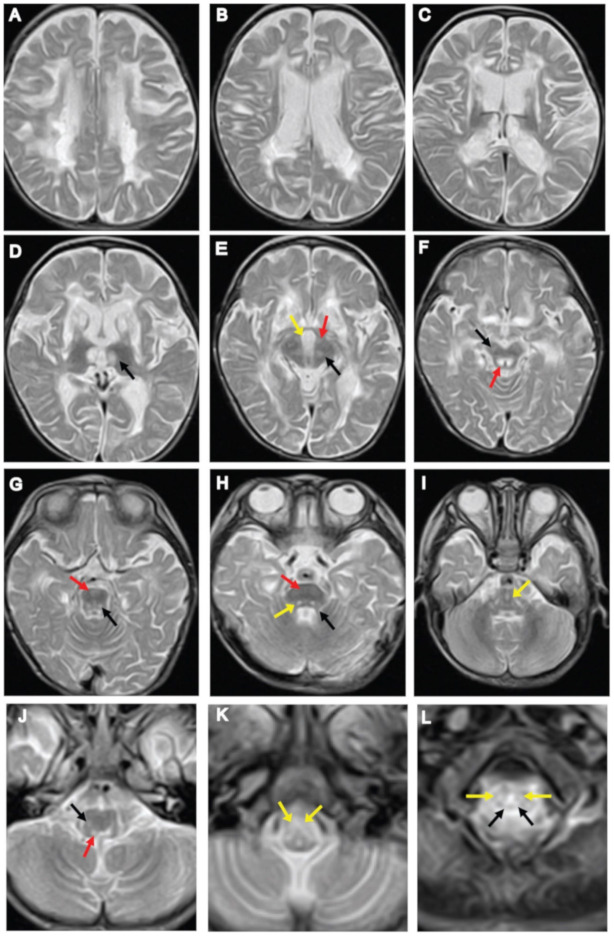
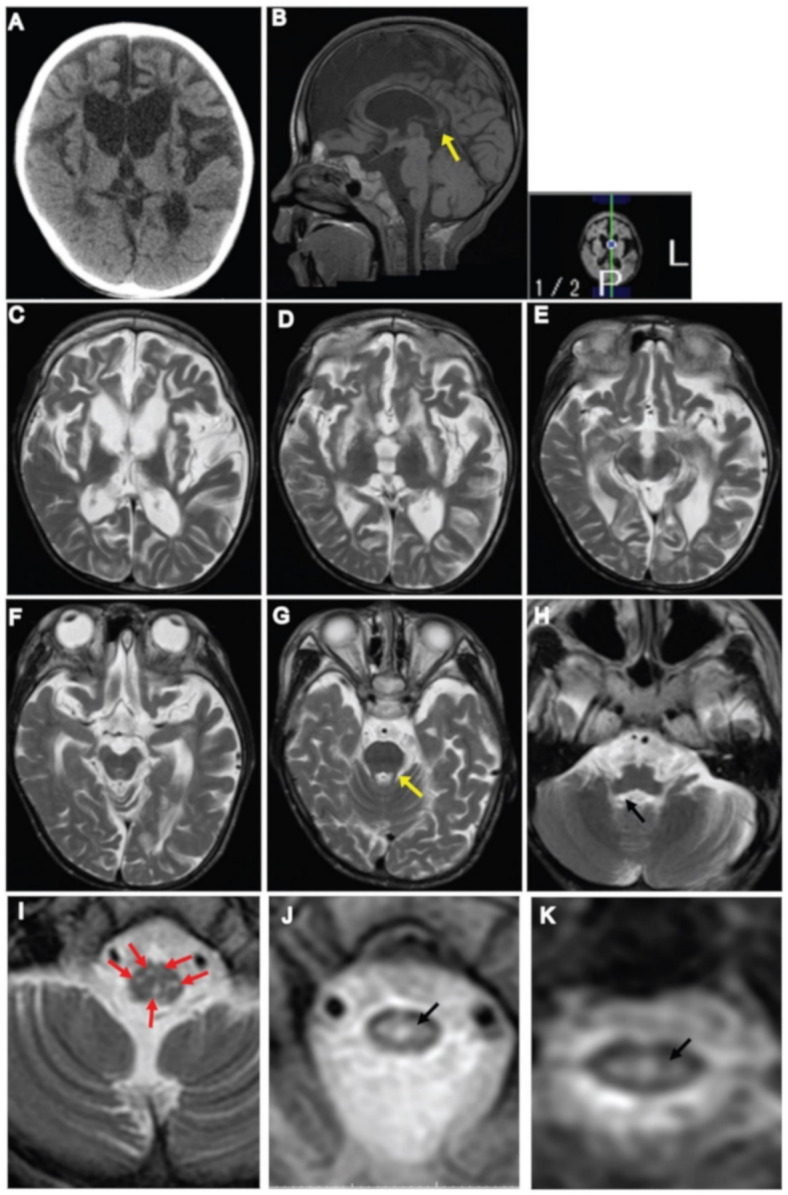
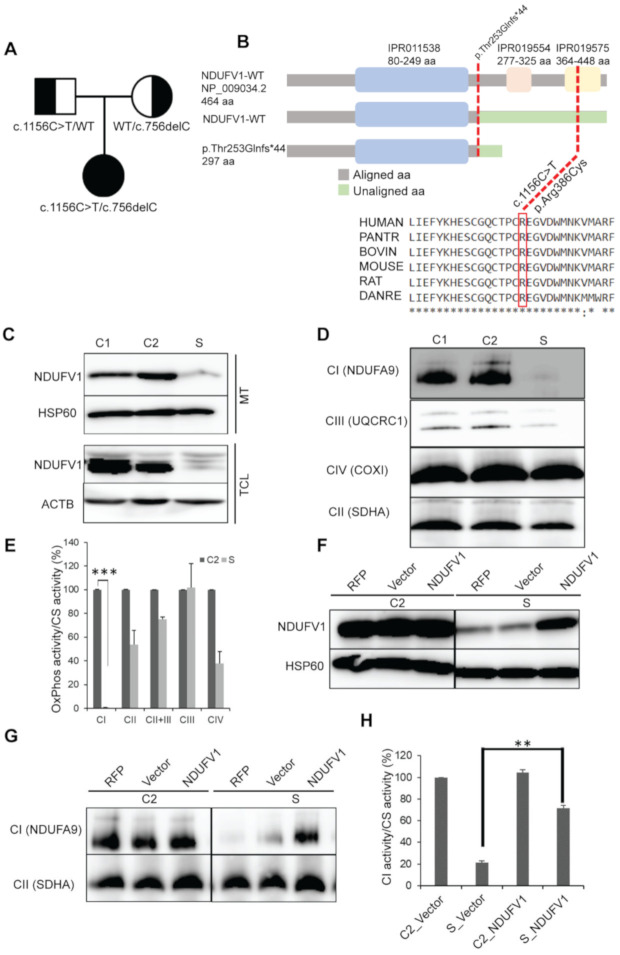
Leigh syndrome (LS) is most frequently characterized by the presence of focal, bilateral, and symmetric brain lesions Leukoencephalopathy with brainstem and spinal cord involvement and lactate elevation (LBSL) is a rare condition, characterized by progressive pyramidal, cerebellar, and dorsal column dysfunction. We describe a case with infantile-onset neurodegeneration, psychomotor retardation, irritability, hypotonia, and nystagmus. Brain MRI demonstrated signal abnormalities in the deep cerebral white matter, corticospinal and dorsal column tracts, and pyramids, which resemble the MRI pattern of a severe form of LBSL, and involvement of basal ganglia and thalamus that resemble the radiological features of LS. We identified biallelic loss-of-function mutations, one novel (c.756delC, p.Thr253Glnfs*44) and another reported (c.1156C > T, p.Arg386Cys), in NDUFV1 (NADH:Ubiquinone Oxidoreductase Core Subunit V1) by exome sequencing. Biochemical and functional analyses revealed lactic acidosis, complex I (CI) assembly and enzyme deficiency, and a loss of NDUFV1 protein. Complementation assays restored the NDUFV1 protein, CI assembly, and CI enzyme levels. The clinical and radiological features of this case are compatible with the phenotype of LS and LBSL associated with NDUFV1 mutations.
Keywords: Leigh syndrome; NDUFV1; OxPhos deficiency; leukodystrophy; leukoencephalopathy with brainstem and spinal cord involvement and lactate elevation.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Leukoencephalopathy with brainstem and spinal cord involvement and lactate elevation (LBSL): assessment of the involved white matter tracts by MRI.Eur J Radiol. 2014 Jan;83(1):191-6. doi: 10.1016/j.ejrad.2013.09.023. Eur J Radiol. 2014. PMID: 24558666
-
The first pediatric case of leukoencephalopathy with brainstem and spinal cord involvement and lactate elevation (LBSL) from Turkey.Turk J Pediatr. 2018;60(2):216-220x. doi: 10.24953/turkjped.2018.02.018. Turk J Pediatr. 2018. PMID: 30325133
-
Leigh syndrome associated with mitochondrial complex I deficiency due to novel mutations In NDUFV1 and NDUFS2.Gene. 2013 Mar 1;516(1):162-7. doi: 10.1016/j.gene.2012.12.024. Epub 2012 Dec 22. Gene. 2013. PMID: 23266820
-
NDUFV1-Related Mitochondrial Complex-1 Disorders: A Retrospective Case Series and Literature Review.Pediatr Neurol. 2024 Jun;155:91-103. doi: 10.1016/j.pediatrneurol.2024.02.012. Epub 2024 Mar 6. Pediatr Neurol. 2024. PMID: 38626668 Review.
-
Adult-onset leukoencephalopathy with brain stem and spinal cord involvement in Chinese Han population: a case report and literature review.Neurol India. 2013 Mar-Apr;61(2):161-3. doi: 10.4103/0028-3886.111123. Neurol India. 2013. PMID: 23644316 Review.
Cited by
-
The neuropathologic findings in a case of progressive cavitating leukoencephalopathy due to NDUFV1 pathogenic variants.Acta Neuropathol Commun. 2022 Sep 26;10(1):142. doi: 10.1186/s40478-022-01445-1. Acta Neuropathol Commun. 2022. PMID: 36163075 Free PMC article.
-
Mitochondrial protein dysfunction in pathogenesis of neurological diseases.Front Mol Neurosci. 2022 Sep 7;15:974480. doi: 10.3389/fnmol.2022.974480. eCollection 2022. Front Mol Neurosci. 2022. PMID: 36157077 Free PMC article. Review.
-
Mitochondrial complex I deficiency in a 4-year-old boy due to compound heterozygous NDUFV1 mutation: a case report of a new pathogenic variant.Oxf Med Case Reports. 2025 Apr 8;2025(4):omae166. doi: 10.1093/omcr/omae166. eCollection 2025 Apr. Oxf Med Case Reports. 2025. PMID: 40207266 Free PMC article.
-
NDUFV1 attenuates renal ischemia-reperfusion injury by improving mitochondrial homeostasis.J Cell Mol Med. 2023 May;27(10):1341-1352. doi: 10.1111/jcmm.17735. Epub 2023 Apr 7. J Cell Mol Med. 2023. PMID: 37029501 Free PMC article.
-
Comprehensive analysis of lactate-related gene profiles and immune characteristics in lupus nephritis.Front Immunol. 2024 Feb 22;15:1329009. doi: 10.3389/fimmu.2024.1329009. eCollection 2024. Front Immunol. 2024. PMID: 38455045 Free PMC article.
References
-
- Ortega-Recalde O., Fonseca D.J., Patino L.C., Atuesta J.J., Rivera-Nieto C., Restrepo C.M., Mateus H.E., van der Knaap M.S., Laissue P. A novel familial case of diffuse leukodystrophy related to NDUFV1 compound heterozygous mutations. Mitochondrion. 2013;13:749–754. doi: 10.1016/j.mito.2013.03.010. - DOI - PubMed
-
- Vilain C., Rens C., Aeby A., Baleriaux D., Van Bogaert P., Remiche G., Smet J., Van Coster R., Abramowicz M., Pirson I. A novel NDUFV1 gene mutation in complex I deficiency in consanguineous siblings with brainstem lesions and Leigh syndrome. Clin. Genet. 2012;82:264–270. doi: 10.1111/j.1399-0004.2011.01743.x. - DOI - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
