

Recurrence Risk after Radical Colorectal Cancer Surgery-Less Than before, But How High Is It?
- PMID: 33182510
- PMCID: PMC7696064
- DOI: 10.3390/cancers12113308
Recurrence Risk after Radical Colorectal Cancer Surgery-Less Than before, But How High Is It?
Abstract
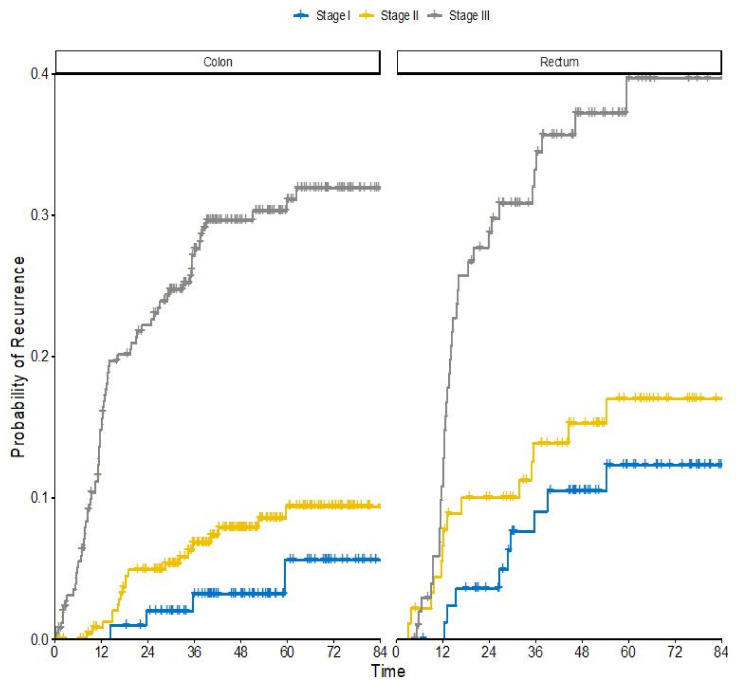
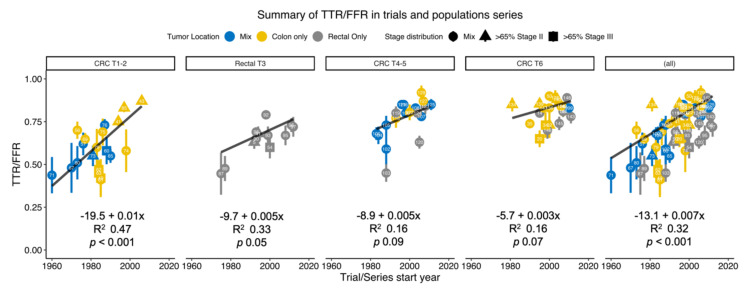
Adjuvant chemotherapy aims at eradicating tumour cells sometimes present after radical surgery for a colorectal cancer (CRC) and thereby diminish the recurrence rate and prolong time to recurrence (TTR). Remaining tumour cells will lead to recurrent disease that is usually fatal. Adjuvant therapy is administered based upon the estimated recurrence risk, which in turn defines the need for this treatment. This systematic overview aims at describing whether the need has decreased since trials showing that adjuvant chemotherapy provides benefits in colon cancer were performed decades ago. Thanks to other improvements than the administration of adjuvant chemotherapy, such as better staging, improved surgery, the use of radiotherapy and more careful pathology, recurrence risks have decreased. Methodological difficulties including intertrial comparisons decades apart and the present selective use of adjuvant therapy prevent an accurate estimate of the magnitude of the decreased need. Furthermore, most trials do not report recurrence rates or TTR, only disease-free and overall survival (DFS/OS). Fewer colon cancer patients, particularly in stage II but also in stage III, today display a sufficient need for adjuvant treatment considering the burden of treatment, especially when oxaliplatin is added. In rectal cancer, neo-adjuvant treatment will be increasingly used, diminishing the need for adjuvant treatment.
Keywords: adjuvant treatment; chemotherapy; colon cancer; colorectal cancer; rectal cancer; recurrence risk; systematic overview.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Schmoll H.J., Van Cutsem E., Stein A., Valentini V., Glimelius B., Haustermans K., Nordlinger B., van de Velde C.J., Balmana J., Regula J., et al. ESMO Consensus Guidelines for management of patients with colon and rectal cancer. a personalized approach to clinical decision making. Ann. Oncol. 2012;23:2479–2516. doi: 10.1093/annonc/mds236. - DOI - PubMed
-
- Argiles G., Tabernero J., Labianca R., Hochhauser D., Salazar R., Iveson T., Laurent-Puig P., Quirke P., Yoshino T., Taieb J., et al. Localised colon cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2020 doi: 10.1016/j.annonc.2020.06.022. In press. - DOI - PubMed
-
- NCCN Guidelines Colon Cancer, Version 3. [(accessed on 23 May 2020)];2020 Available online: www.NCCN.org.
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
