

Systematic Review with Meta-Analysis: Endoscopic and Surgical Resection for Ampullary Lesions
- PMID: 33182806
- PMCID: PMC7696506
- DOI: 10.3390/jcm9113622
Systematic Review with Meta-Analysis: Endoscopic and Surgical Resection for Ampullary Lesions
Abstract
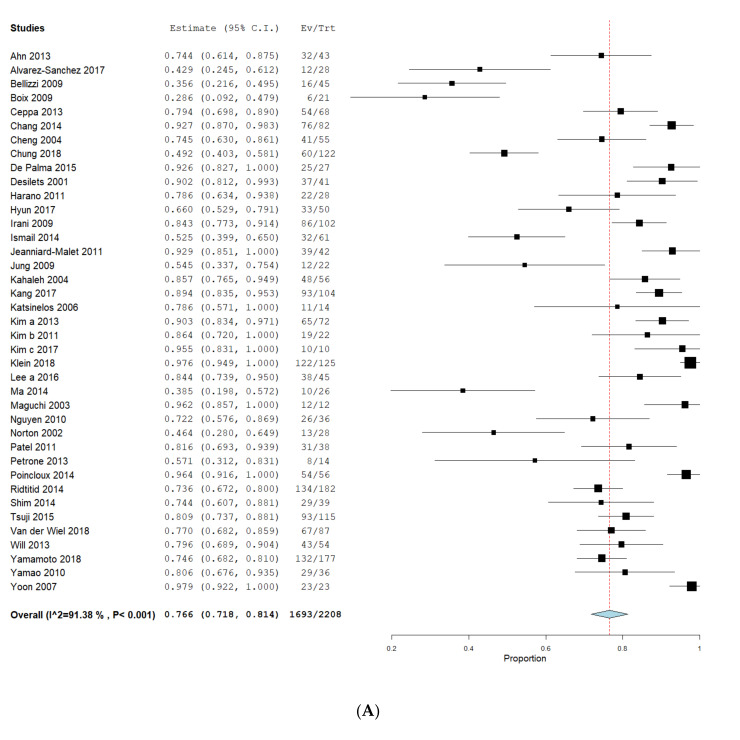
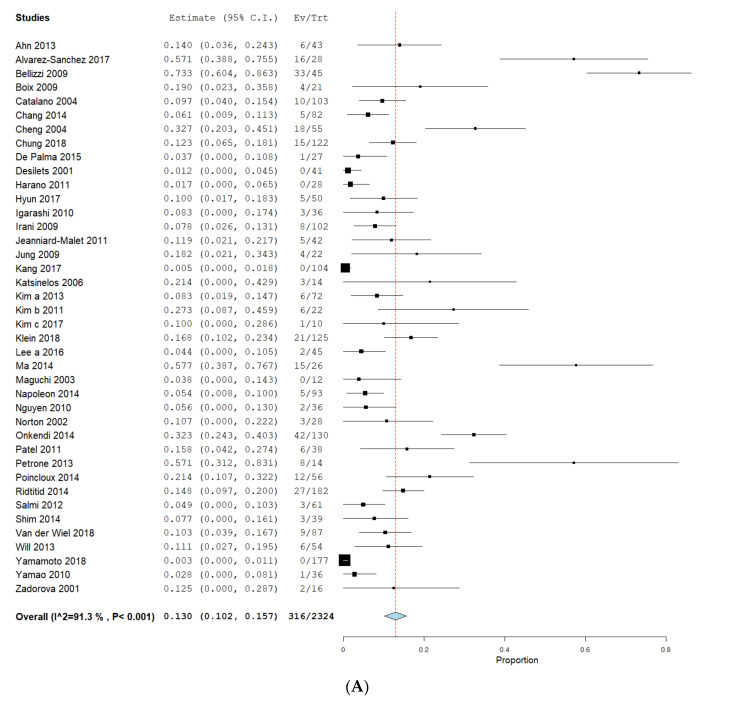
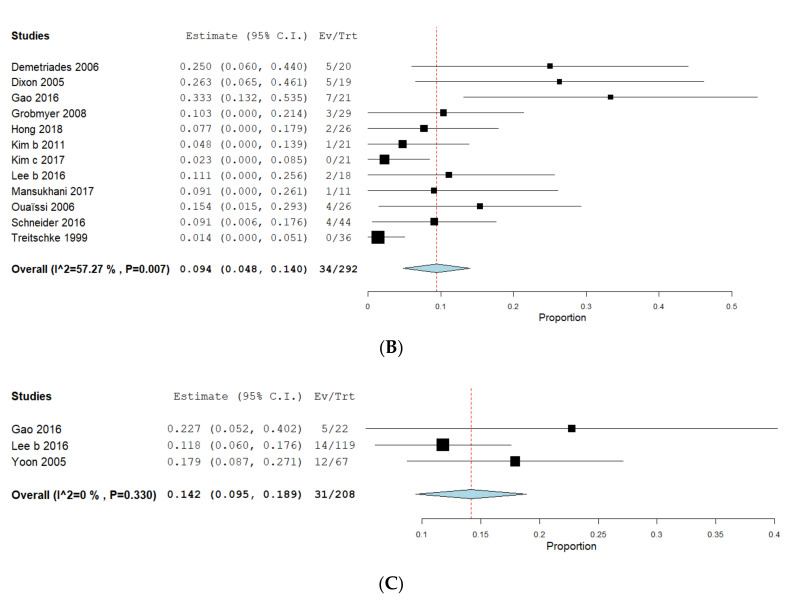
Ampullary lesions (ALs) can be treated by endoscopic (EA) or surgical ampullectomy (SA) or pancreaticoduodenectomy (PD). However, EA carries significant risk of incomplete resection while surgical interventions can lead to substantial morbidity. We performed a systematic review and meta-analysis for R0, adverse-events (AEs) and recurrence between EA, SA and PD. Electronic databases were searched from 1990 to 2018. Outcomes were calculated as pooled means using fixed and random-effects models and the Freeman-Tukey-Double-Arcsine-Proportion-model. We identified 59 independent studies. The pooled R0 rate was 76.6% (71.8-81.4%, I2 = 91.38%) for EA, 96.4% (93.6-99.2%, I2 = 37.8%) for SA and 98.9% (98.0-99.7%, I2 = 0%) for PD. AEs were 24.7% (19.8-29.6%, I2 = 86.4%), 28.3% (19.0-37.7%, I2 = 76.8%) and 44.7% (37.9-51.4%, I2 = 0%), respectively. Recurrences were registered in 13.0% (10.2-15.6%, I2 = 91.3%), 9.4% (4.8-14%, I2 = 57.3%) and 14.2% (9.5-18.9%, I2 = 0%). Differences between proportions were significant in R0 for EA compared to SA (p = 0.007) and PD (p = 0.022). AEs were statistically different only between EA and PD (p = 0.049) and recurrence showed no significance for EA/SA or EA/PD. Our data indicate an increased rate of complete resection in surgical interventions accompanied with a higher risk of complications. However, studies showed various sources of bias, limited quality of data and a significant heterogeneity, particularly in EA studies.
Keywords: ampulla of Vater; ampullectomy; pancreaticoduodenectomy; papillectomy; trans-duodenal ampullectomy.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures




References
-
- Gibbs E.R., Walton G.F., Kent R.B., 3rd, Laws H.L. Villous tumors of the ampulla Vater. Am. Surg. 1997;63:467–471. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
