

Anastomosis technique for pancreatojejunostomy and early removal of drainage tubes may reduce postoperative pancreatic fistula
- PMID: 33183313
- PMCID: PMC7661166
- DOI: 10.1186/s12957-020-02067-4
Anastomosis technique for pancreatojejunostomy and early removal of drainage tubes may reduce postoperative pancreatic fistula
Abstract
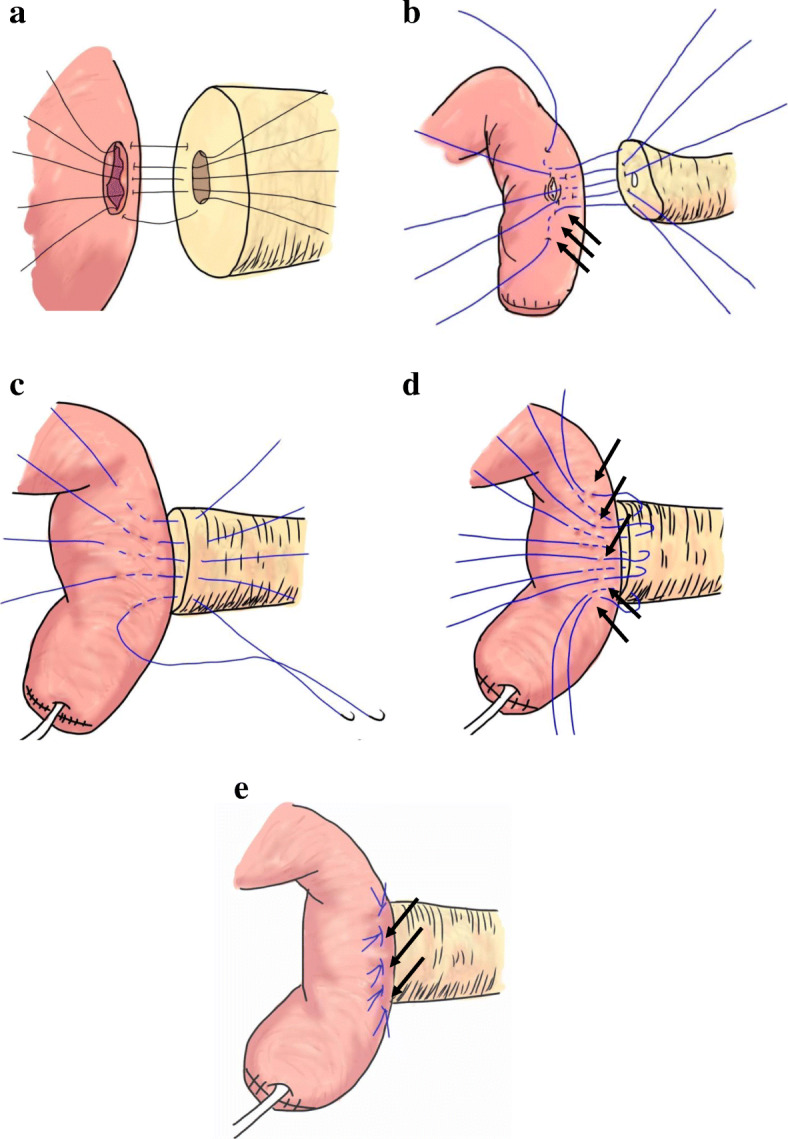
Background: Postoperative pancreatic fistula (POPF) is one of the most serious complications after pancreaticoduodenectomy (PD). Various factors have been reported as POPF risks, but the most serious of these is soft pancreas. To reduce POPF occurrences, many changes to the PD process have been proposed. This study evaluates short-term results of anastomosis technique for PD.
Methods: In total, 123 patients with soft pancreases who had undergone PD at Yamanashi University between January 2012 and August 2020 were retrospectively analyzed. We divided these patients into two groups depending on the time PD was performed: a conventional group (n = 67) and a modified group (n = 56).
Results: The rate of clinically relevant POPF was significantly lower in the modified group than that in the conventional group (5.4% vs 22.4%, p value < 0.001), with there being only one case of POPF in the modified group. There were no cases of POPF-related hemorrhaging in the modified group. On the third day after the operation, the amylase levels in the drainage fluid for the modified group became less than half (1696 vs 650 U/L). Multivariate analysis showed that the modified method was the independent predictors to prevent clinical POPF (p value = 0.002).
Conclusions: Our novel anastomosis technique for pancreatojejunostomy reduced POPF in PD, especially in cases where the patient had a soft pancreas.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
The individualized selection of Pancreaticoenteric anastomosis in Pancreaticoduodenectomy.BMC Surg. 2020 Jun 22;20(1):140. doi: 10.1186/s12893-020-00791-y. BMC Surg. 2020. PMID: 32571289 Free PMC article.
-
Modified Pancreatojejunostomy in Pancreaticoduodenectomy for the Treatment of Periampullary Tumor: 8 Years of Surgical Experience.Med Sci Monit. 2019 May 21;25:3788-3795. doi: 10.12659/MSM.916837. Med Sci Monit. 2019. PMID: 31112531 Free PMC article.
-
Drainage posterior to pancreaticojejunostomy reduces the severity of postoperative pancreatic fistula after pancreaticoduodenectomy.World J Surg Oncol. 2024 Nov 27;22(1):315. doi: 10.1186/s12957-024-03597-x. World J Surg Oncol. 2024. PMID: 39605037 Free PMC article.
-
Surgical techniques and postoperative management to prevent postoperative pancreatic fistula after pancreatic surgery.World J Gastroenterol. 2019 Jul 28;25(28):3722-3737. doi: 10.3748/wjg.v25.i28.3722. World J Gastroenterol. 2019. PMID: 31391768 Free PMC article. Review.
-
Pancreaticodigestive anastomosis and the postoperative management strategies to prevent postoperative pancreatic fistula formation after pancreaticoduodenectomy.Surg Today. 2014 Jul;44(7):1207-13. doi: 10.1007/s00595-013-0662-x. Epub 2013 Jul 11. Surg Today. 2014. PMID: 23842691
Cited by
-
Novel end-to-side one-layer continuous pancreaticojejunostomy vs. end-to-end invaginated pancreaticojejunostomy in pancreatoduodenectomy: A single-center retrospective study.Front Surg. 2023 Jan 6;9:980056. doi: 10.3389/fsurg.2022.980056. eCollection 2022. Front Surg. 2023. PMID: 36684316 Free PMC article.
-
Pancreatic outflow tract reconstruction after pancreaticoduodenectomy: a meta-analysis of randomized controlled trials.World J Surg Oncol. 2021 Jul 6;19(1):203. doi: 10.1186/s12957-021-02314-2. World J Surg Oncol. 2021. PMID: 34229720 Free PMC article. Review.
-
AutoFRS: an externally validated, annotation-free approach to computational preoperative complication risk stratification in pancreatic surgery - an experimental study.Int J Surg. 2025 May 1;111(5):3212-3223. doi: 10.1097/JS9.0000000000002327. Int J Surg. 2025. PMID: 40146236 Free PMC article.
-
Prediction of clinically relevant postoperative pancreatic fistula using radiomic features and preoperative data.Sci Rep. 2023 May 9;13(1):7506. doi: 10.1038/s41598-023-34168-x. Sci Rep. 2023. PMID: 37161007 Free PMC article.
-
Drainage volume on postoperative day one to predict clinically relevant postoperative pancreatic fistula following distal pancreatectomy.BMC Surg. 2022 Aug 1;22(1):297. doi: 10.1186/s12893-022-01748-z. BMC Surg. 2022. PMID: 35909183 Free PMC article.
References
-
- Kimura W, Miyata H, Gotoh M, Hirai I, Kenjo A, Kitagawa Y, et al. A pancreaticoduodenectomy risk model derived from 8575 cases from a national single-race population (Japanese) using a web-based data entry system: the 30-day and in-hospital mortality rates for pancreaticoduodenectomy. Ann Surg. 2014;259:773–780. doi: 10.1097/SLA.0000000000000263. - DOI - PubMed
-
- Bassi C, Marchegiani G, Dervenis C, Sarr M, Abu Hilal M, Adham M, et al. International study group on pancreatic surgery (ISGPS), the 2016 update of the international study group (ISGPS) definition and grading of postoperative pancreatic fistula: 11 years after. Surgery. 2017;161:584–591. doi: 10.1016/j.surg.2016.11.014. - DOI - PubMed
-
- Keck T, Wellner UF, Bahra M, Klein F, Sick O, Niedergethmann M, et al. Pancreatogastrostomy versus pancreatojejunostomy for reconstruction after pancreatoduodenectomy (RECOPANC, DRKS 00000767): perioperative and long-term results of a multicenter randomized controlled trial. Ann Surg. 2016;263:440–449. doi: 10.1097/SLA.0000000000001240. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
