

Delirium
- PMID: 33184265
- PMCID: PMC9012267
- DOI: 10.1038/s41572-020-00223-4
Delirium
Erratum in
-
Publisher Correction: Delirium.Nat Rev Dis Primers. 2020 Dec 1;6(1):94. doi: 10.1038/s41572-020-00236-z. Nat Rev Dis Primers. 2020. PMID: 33262366
Abstract
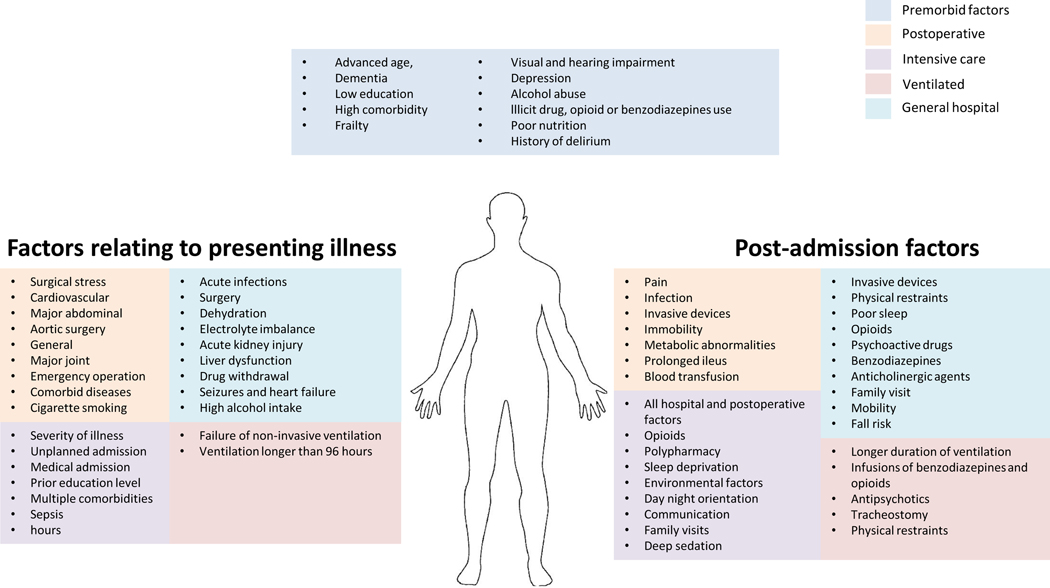
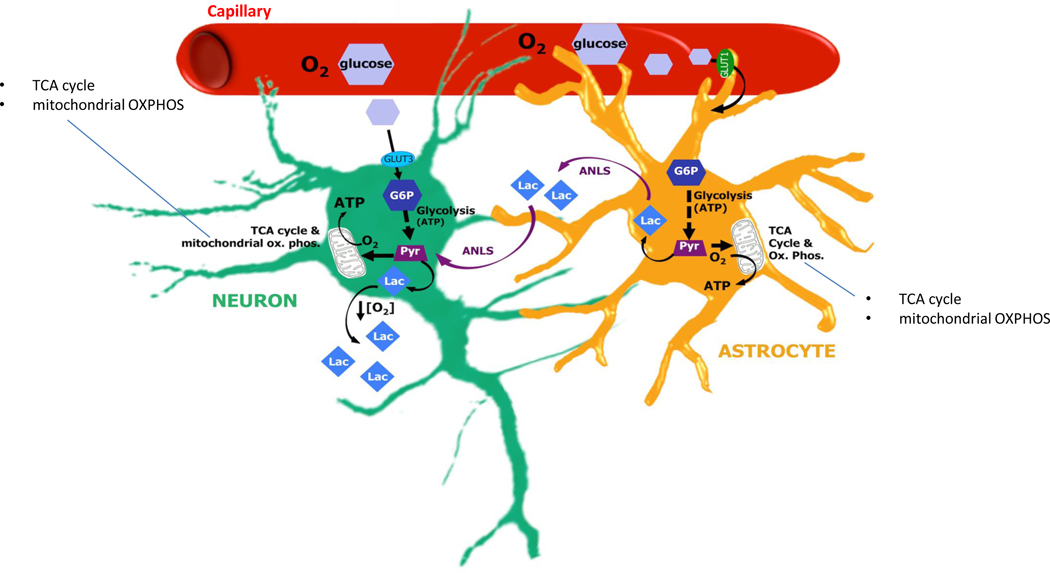
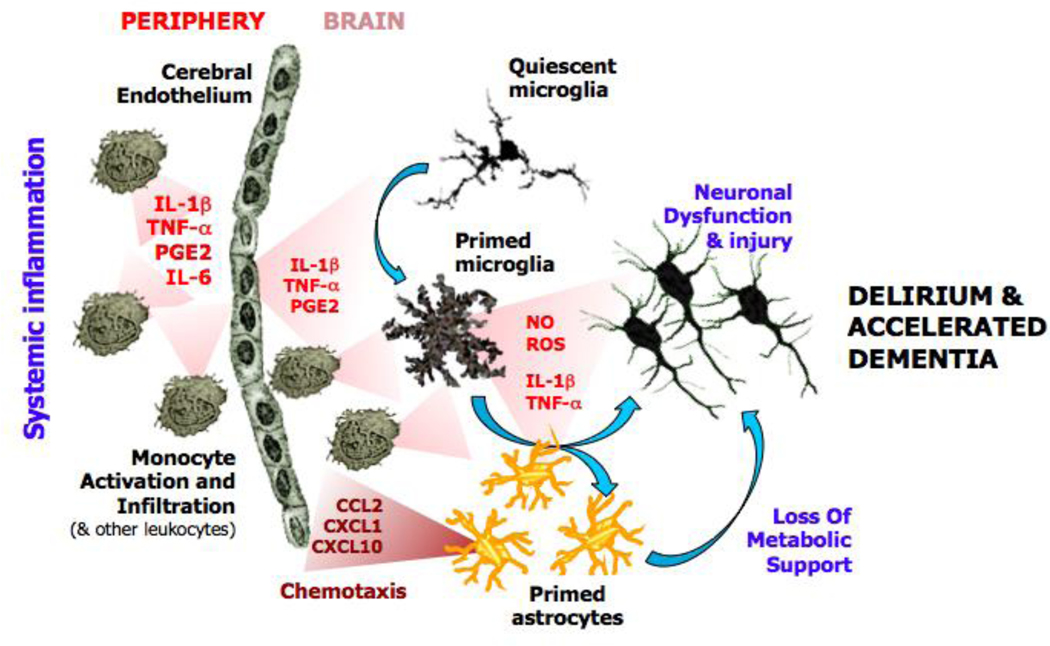
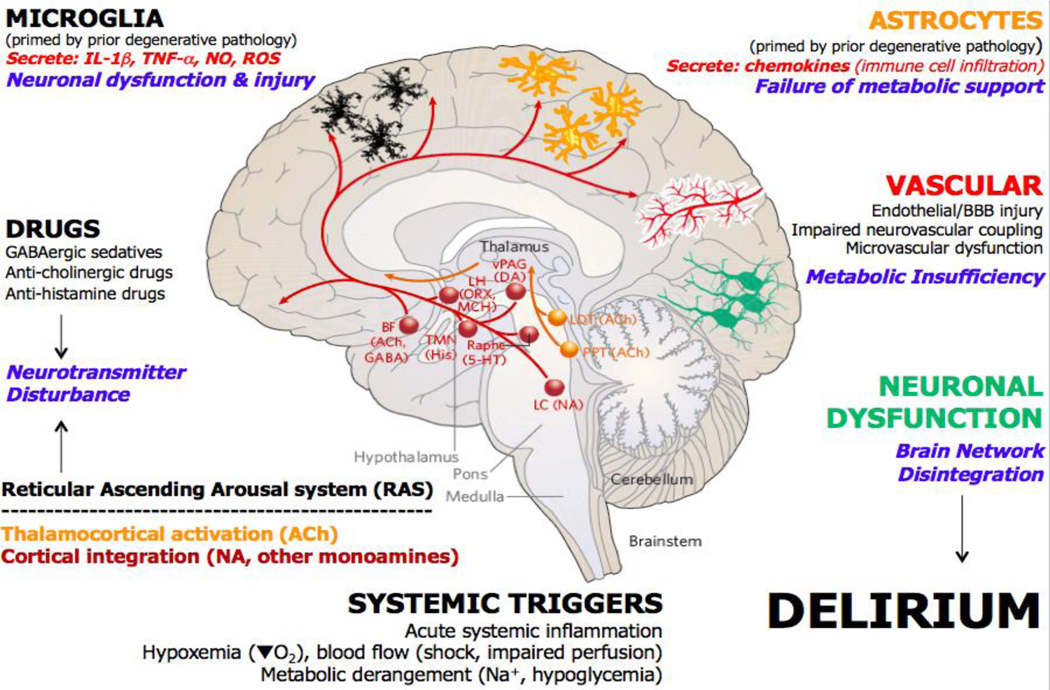
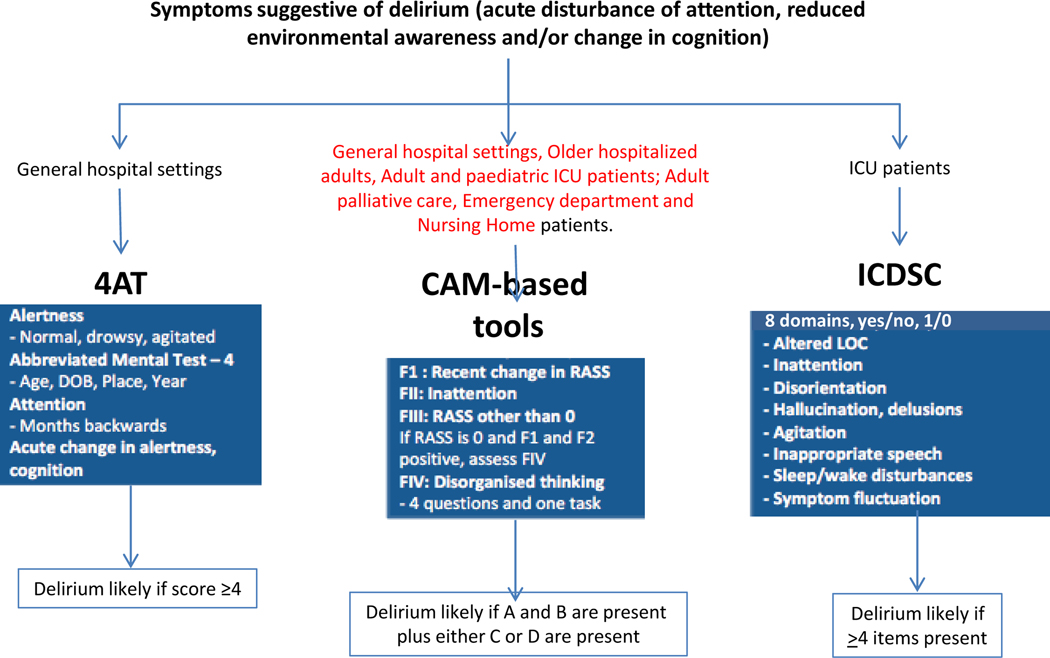
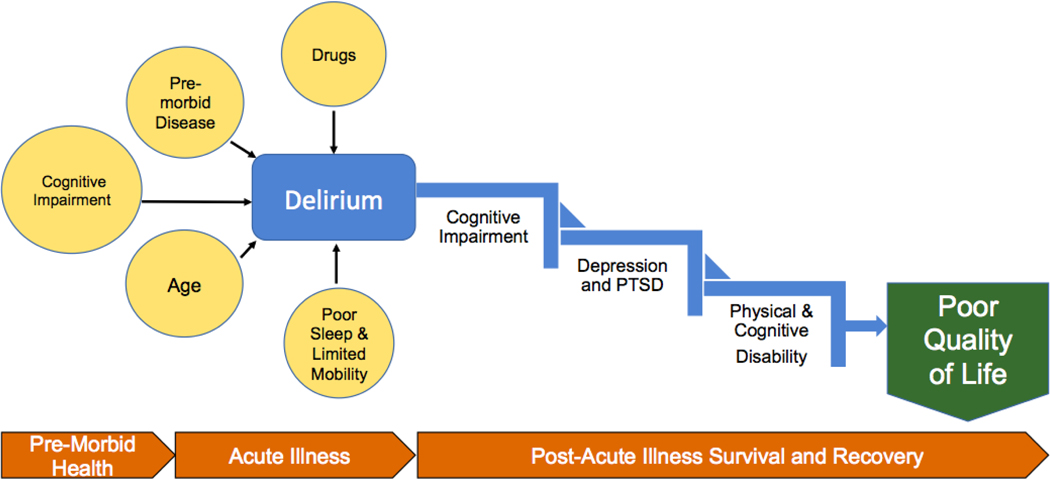
Delirium, a syndrome characterized by an acute change in attention, awareness and cognition, is caused by a medical condition that cannot be better explained by a pre-existing neurocognitive disorder. Multiple predisposing factors (for example, pre-existing cognitive impairment) and precipitating factors (for example, urinary tract infection) for delirium have been described, with most patients having both types. Because multiple factors are implicated in the aetiology of delirium, there are likely several neurobiological processes that contribute to delirium pathogenesis, including neuroinflammation, brain vascular dysfunction, altered brain metabolism, neurotransmitter imbalance and impaired neuronal network connectivity. The Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-5) is the most commonly used diagnostic system upon which a reference standard diagnosis is made, although many other delirium screening tools have been developed given the impracticality of using the DSM-5 in many settings. Pharmacological treatments for delirium (such as antipsychotic drugs) are not effective, reflecting substantial gaps in our understanding of its pathophysiology. Currently, the best management strategies are multidomain interventions that focus on treating precipitating conditions, medication review, managing distress, mitigating complications and maintaining engagement to environmental issues. The effective implementation of delirium detection, treatment and prevention strategies remains a major challenge for health-care organizations globally.
Figures
References
-
-
Pandharipande PP et al. Long-term cognitive impairment after critical illness. The New England journal of medicine 369, 1306–1316, doi: 10.1056/NEJMoa1301372 (2013).
This prospective longitudinal cohort study demonstrated that critically ill patients are at risk of LTCI after critical illness and that this new LTCI can persist at 3 and 12 months follow up and is associated with duration of delirium.
-
-
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders (DSM-5®). (American Psychiatric Association Publishing, 2013).
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
