

Accelerated ethanol elimination via the lungs
- PMID: 33184355
- PMCID: PMC7665168
- DOI: 10.1038/s41598-020-76233-9
Accelerated ethanol elimination via the lungs
Abstract
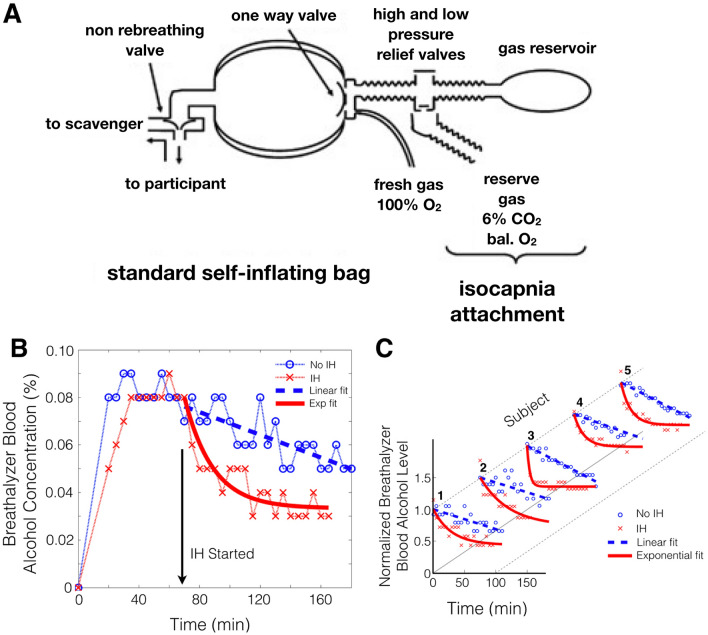
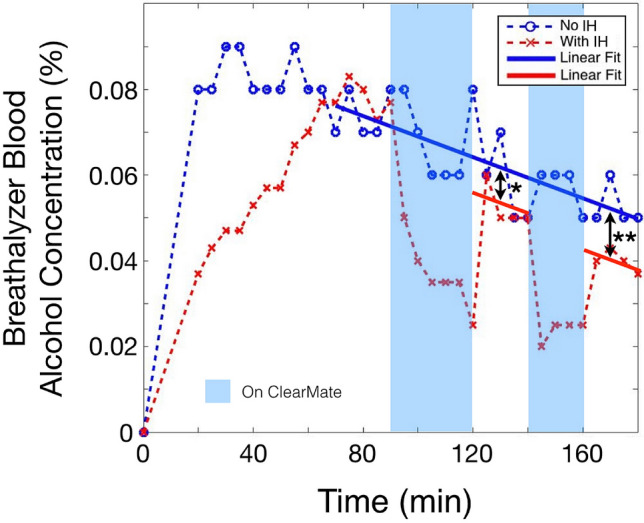
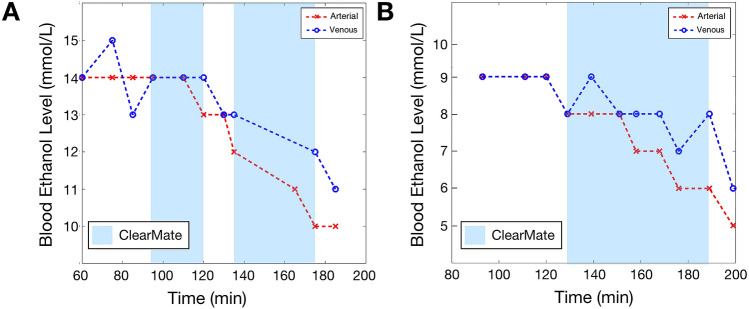
Ethanol poisoning is endemic the world over. Morbidity and mortality depend on blood ethanol levels which in turn depend on the balance between its rates of absorption and clearance. Clearance of ethanol is mostly at a constant rate via enzymatic metabolism. We hypothesized that isocapnic hyperpnea (IH), previously shown to be effective in acceleration of clearance of vapour anesthetics and carbon monoxide, would also accelerate the clearance of ethanol. In this proof-of-concept pilot study, five healthy male subjects were brought to a mildly elevated blood ethanol concentration (~ 0.1%) and ethanol clearance monitored during normal ventilation and IH on different days. IH increased elimination rate of ethanol in proportion to blood levels, increasing the elimination rate more than three-fold. Increased veno-arterial ethanol concentration differences during IH verified the efficacy of ethanol clearance via the lung. These data indicate that IH is a nonpharmacologic means to accelerate the elimination of ethanol by superimposing first order elimination kinetics on underlying zero order liver metabolism. Such kinetics may prove useful in treating acute severe ethanol intoxication.
Conflict of interest statement
Thornhill Medical Inc. developed the ClearMateTM for the treatment of carbon monoxide poisoning and made a unit available on request at no cost for this study. JAF, OS, JD, LF, and DJM are appointees at the University of Toronto and employees of and/or own shares in Thornhill Medical Inc, which is a for profit spin-off from the University Health Network (University of Toronto), which continues to own the IP. JMK, DV, APC, LV, KS, and RH have no competing interests.
Figures
References
-
- Feldman RS, Meyer JS, Quenzer LF. Principles of Neuropsychopharmacology. Sunderland: Sinauer Associates Inc.; 1997.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
