

Dyssynergic patterns of defecation in constipated adolescents and young adults with anorectal malformations
- PMID: 33184420
- PMCID: PMC7661710
- DOI: 10.1038/s41598-020-76841-5
Dyssynergic patterns of defecation in constipated adolescents and young adults with anorectal malformations
Abstract
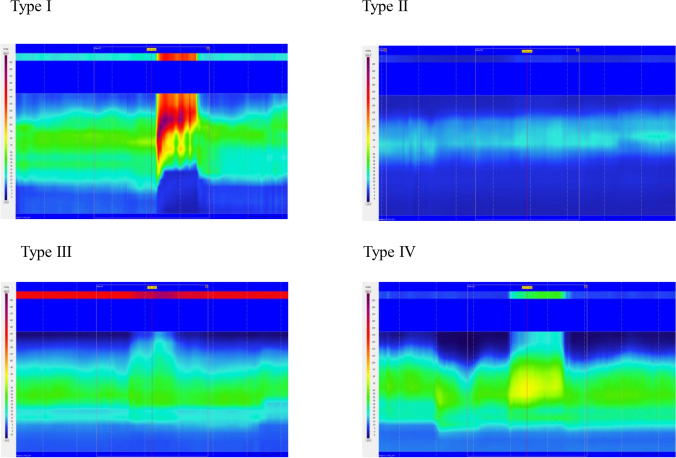
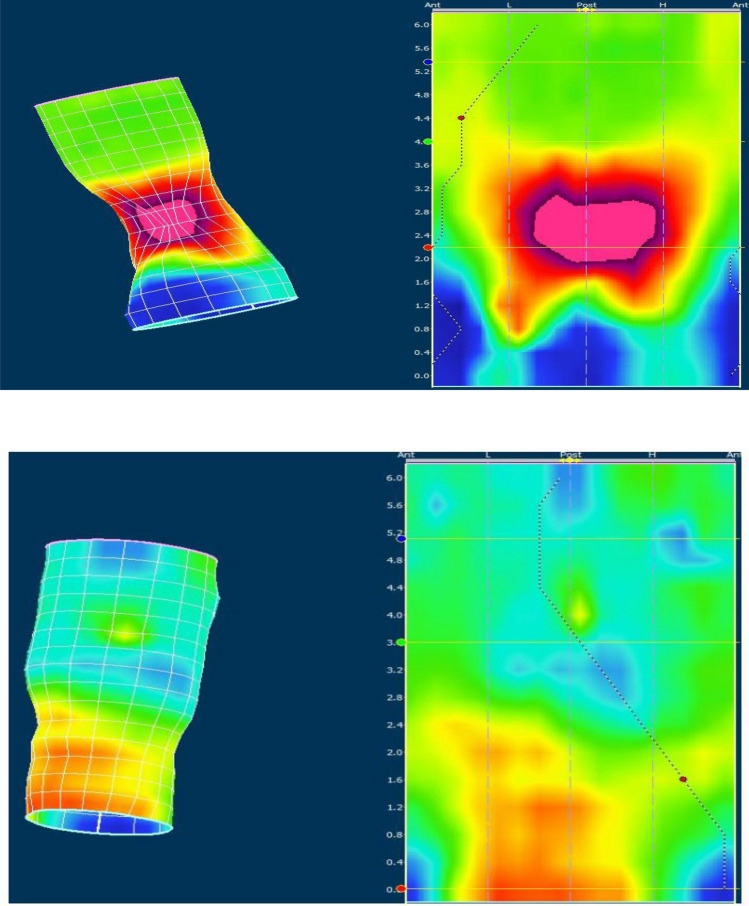
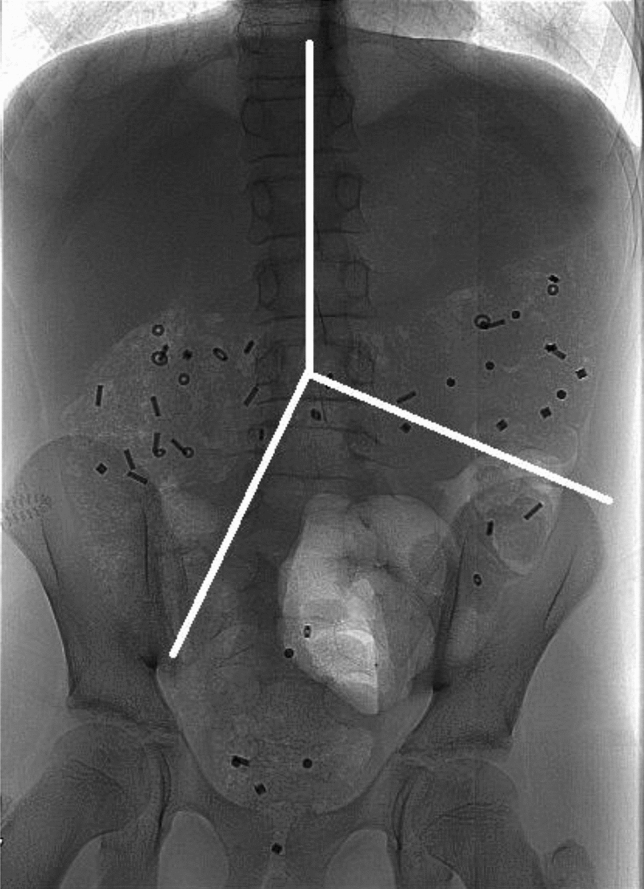
We aimed to evaluate the etiologies of constipation in patients with anorectal malformations having a good prognosis for bowel control but a high risk of constipation. We included twenty-five patients from the Odense university hospital in Denmark. Patients were subjected to colon transit time examination and high resolution anorectal manometry (HRAM). The median age was 18 (14-24) and 48% (12/25) were females. Fifty-two % (13/25) of patients were diagnosed with constipation. Types of anorectal malformation were perineal fistula (9/25), rectovestibular fistula (8/25), rectourethral bulbar fistula (5/25) and no fistula (3/25). No difference in neither total colon transit time nor segmental colon transit times were found based on the presence of constipation. Only four of the constipated patients fulfilled criteria for dyssynergic defecation with a dyssynergic pattern at HRAM and prolonged colon transit time. A Type I dyssynergic pattern was dominant in constipated patients (7/13). A Dyssynergic defecation pattern was due to isolated contraction of puborectalis muscle in 9 out of 13constipated patients. We found a dyssynergic pattern during attempted defecation in patients with anorectal malformations disregarded the presence of constipation. In the majority of constipated patients an isolated contraction of the puborectalis muscle was visualized with HRAM.
Trial registration: ClinicalTrials.gov NCT02624232.
Conflict of interest statement
The authors declare no competing interests.
Figures

Similar articles
-
Chronic idiopathic constipation: more than a simple colonic transit disorder.J Clin Gastroenterol. 2012 Feb;46(2):150-4. doi: 10.1097/MCG.0b013e318231fc64. J Clin Gastroenterol. 2012. PMID: 22011587
-
Dyssynergic defecation may aggravate constipation: results of mostly pediatric cases with congenital anorectal malformation.Am J Surg. 2015 Aug;210(2):357-64. doi: 10.1016/j.amjsurg.2014.09.038. Epub 2015 Jan 31. Am J Surg. 2015. PMID: 25721649
-
Prevalence and pathophysiology of functional constipation among women in Catalonia, Spain.Dis Colon Rectum. 2011 Dec;54(12):1560-9. doi: 10.1097/DCR.0b013e31822cb5c2. Dis Colon Rectum. 2011. PMID: 22067186
-
Anorectal manometry to diagnose dyssynergic defecation: Systematic review and meta-analysis of diagnostic test accuracy.Neurogastroenterol Motil. 2021 Nov;33(11):e14137. doi: 10.1111/nmo.14137. Epub 2021 Mar 27. Neurogastroenterol Motil. 2021. PMID: 33772969 Free PMC article.
-
Clinical utility of colonic and anorectal manometry in chronic constipation.J Clin Gastroenterol. 2010 Oct;44(9):597-609. doi: 10.1097/MCG.0b013e3181e88532. J Clin Gastroenterol. 2010. PMID: 20679903 Review.
Cited by
-
Evaluation of Anal Sphincter with High Resolution Anorectal Manometry and 3D Reconstruction in Patients with Anorectal Malformation.Children (Basel). 2023 Jun 9;10(6):1037. doi: 10.3390/children10061037. Children (Basel). 2023. PMID: 37371268 Free PMC article.
-
Diagnosis and management of fecal incontinence in children and adolescents.Front Pediatr. 2022 Oct 18;10:1034240. doi: 10.3389/fped.2022.1034240. eCollection 2022. Front Pediatr. 2022. PMID: 36330370 Free PMC article. Review.
-
Correlation between congenital pelvic floor muscle development assessed by magnetic resonance imaging and postoperative defecation.Pediatr Surg Int. 2024 Apr 10;40(1):104. doi: 10.1007/s00383-024-05691-3. Pediatr Surg Int. 2024. PMID: 38600320
-
Analysis of factors associated with postoperative complications after primary hypospadias repair: a retrospective study.Transl Androl Urol. 2022 Nov;11(11):1577-1585. doi: 10.21037/tau-22-691. Transl Androl Urol. 2022. PMID: 36507491 Free PMC article.
-
Muscle regeneration therapy using dedifferentiated fat cell (DFAT) for anal sphincter dysfunction.Pediatr Surg Int. 2024 Aug 21;40(1):238. doi: 10.1007/s00383-024-05812-y. Pediatr Surg Int. 2024. PMID: 39167102
References
-
- Borg H, Holmdahl G, Doroszkievicz M, Sillen U. Longitudinal study of lower urinary tract function in children with anorectal malformation. Eur. J. Pediatr. Surg. 2013;24:492–499. - PubMed
-
- Diseth TH, Emblem R. Long-term psychosocial consequences of surgical congenital malformations. Semin. Pediatr. Surg. 2017;26:286–294. - PubMed
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
