

Effects of oral semaglutide on energy intake, food preference, appetite, control of eating and body weight in subjects with type 2 diabetes
- PMID: 33184979
- PMCID: PMC7839771
- DOI: 10.1111/dom.14255
Effects of oral semaglutide on energy intake, food preference, appetite, control of eating and body weight in subjects with type 2 diabetes
Abstract
Aim: To evaluate the effect of oral semaglutide on energy intake and appetite in subjects with type 2 diabetes (T2D).
Materials and methods: In this randomized, double-blind, placebo-controlled, two-period cross-over trial, 15 subjects with T2D received 12 weeks of treatment with once-daily oral semaglutide (4-week dose escalation from 3 to 7 to 14 mg) followed by placebo, or vice versa. Energy intake was measured during an ad libitum lunch, evening meal and snack box after a standard breakfast. Appetite ratings were measured using a visual analogue scale after standard and fat-rich breakfasts. Other assessments included eating and craving control (using the Control of Eating Questionnaire), and changes in body weight and composition.
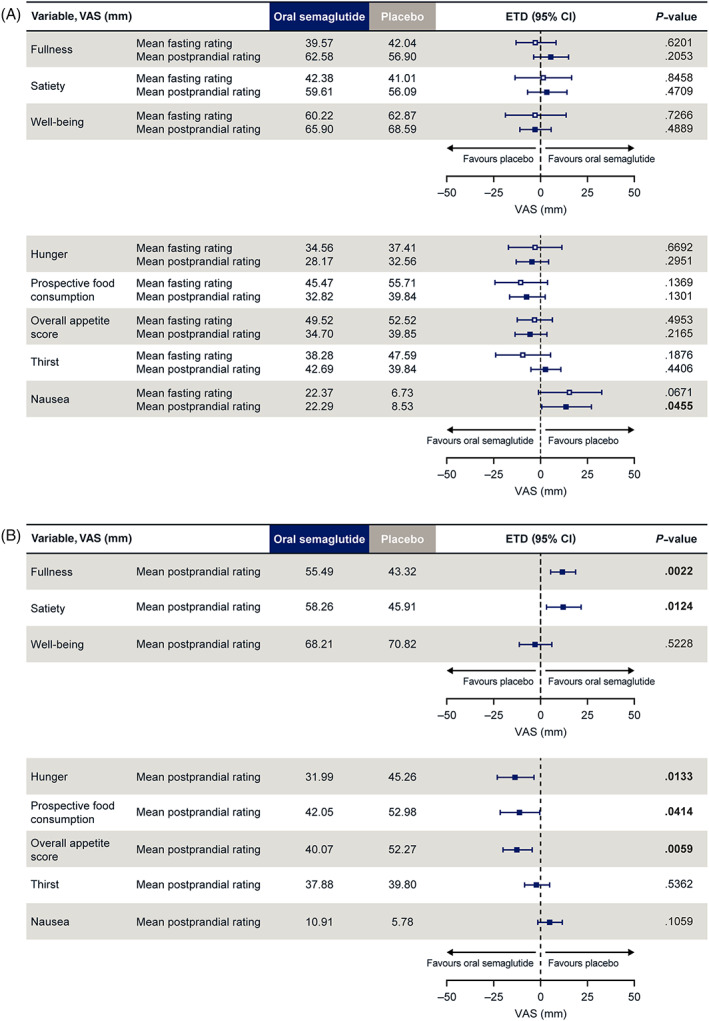
Results: Following a standard breakfast, total daily ad libitum energy intake was significantly lower (38.9%) with oral semaglutide versus placebo in 13 evaluable subjects (estimated treatment difference, -5096.0 kJ; 95% CI -7000.0, -3192.1; P = .0001). After a fat-rich breakfast, there were significant differences in favour of oral semaglutide versus placebo for measures of satiety, hunger and for overall appetite score, with no significant differences following a standard breakfast. Fewer food cravings and better eating control were seen with oral semaglutide versus placebo. Overall, mean body weight decreased by 2.7 kg with oral semaglutide and 0.1 kg with placebo, mostly attributable to body fat mass loss.
Conclusion: After 12 weeks of treatment, ad libitum energy intake was lower with oral semaglutide versus placebo, resulting in reduced body fat mass, and was associated with increased satiety and fullness after a fat-rich breakfast, and improved eating control.
Trial registration number: NCT02773381.
Keywords: GLP-1 analogue; appetite control; body composition; energy regulation; incretin therapy; type 2 diabetes.
© 2020 The Authors. Diabetes, Obesity and Metabolism published by John Wiley & Sons Ltd.
Conflict of interest statement
JB and CG received research grants from Novo Nordisk for the current study. JB served on a Novo Nordisk Obesity Advisory Board and received personal fees from Novo Nordisk, outside the submitted work. STH, KD, RB and TB are employees, and KD, STH and TB shareholders, of Novo Nordisk A/S, the sponsor of this trial.
Figures

References
-
- Flint A, Raben A, Astrup A, Holst JJ. Glucagon‐like peptide 1 promotes satiety and suppresses energy intake in humans. J Clin Invest. 1998;101:515‐520.
-
- Gutzwiller JP, Drewe J, Göke B, et al. Glucagon‐like peptide‐1 promotes satiety and reduces food intake in patients with diabetes mellitus type 2. Am J Physiol. 1999;276:R1541‐R1544. - PubMed
