

Effects of Different Telemonitoring Strategies on Chronic Heart Failure Care: Systematic Review and Subgroup Meta-Analysis
- PMID: 33185554
- PMCID: PMC7695537
- DOI: 10.2196/20032
Effects of Different Telemonitoring Strategies on Chronic Heart Failure Care: Systematic Review and Subgroup Meta-Analysis
Abstract
Background: Telemonitoring studies in chronic heart failure are characterized by mixed mortality and hospitalization outcomes, which have deterred the uptake of telemonitoring in clinical practice. These mixed outcomes may reflect the diverse range of patient management strategies incorporated in telemonitoring. To address this, we compared the effects of different telemonitoring strategies on clinical outcomes.
Objective: The aim of this systematic review and subgroup meta-analysis was to identify noninvasive telemonitoring strategies attributing to improvements in all-cause mortality or hospitalization outcomes for patients with chronic heart failure.
Methods: We reviewed and analyzed telemonitoring strategies from randomized controlled trials (RCTs) comparing telemonitoring intervention with usual care. For each strategy, we examined whether RCTs that applied the strategy in the telemonitoring intervention (subgroup 1) resulted in a significantly lower risk ratio (RR) of all-cause mortality or incidence rate ratio (IRR) of all-cause hospitalization compared with RCTs that did not apply this strategy (subgroup 2).
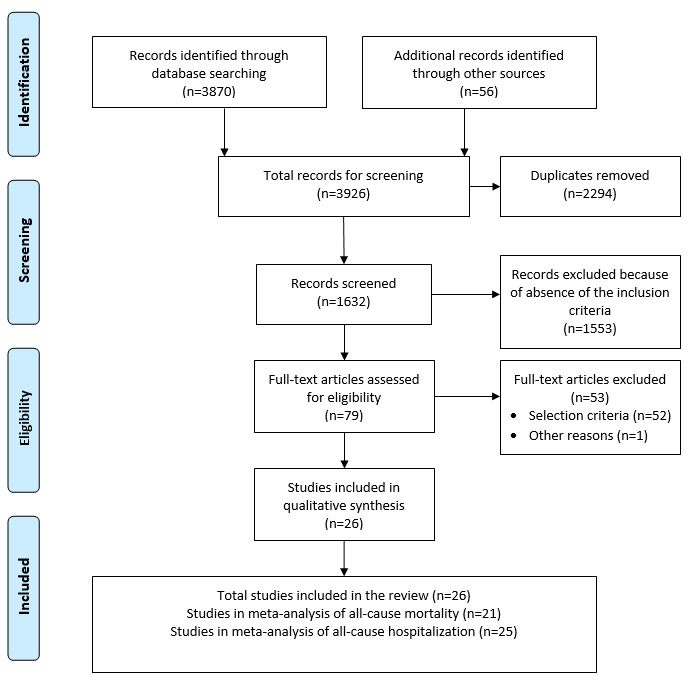
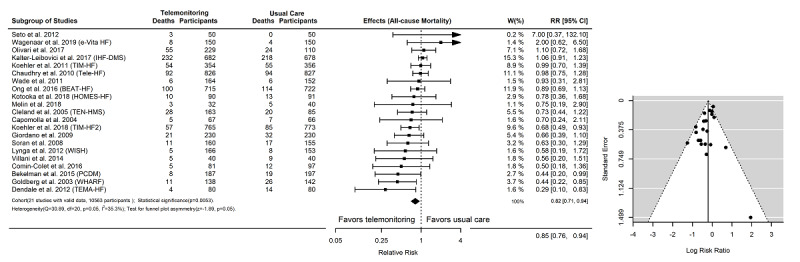
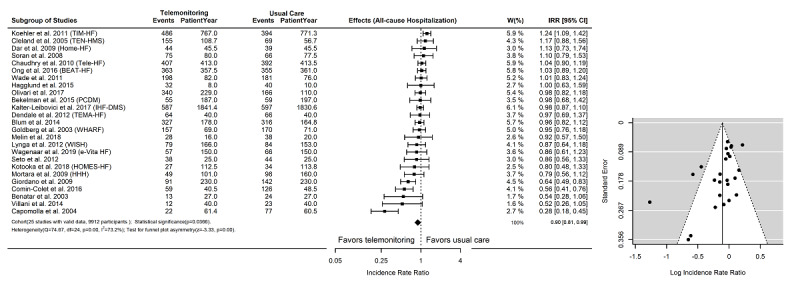
Results: We included 26 RCTs (N=11,450) incorporating 18 different telemonitoring strategies. RCTs that provided medication support were found to be associated with a significantly lower IRR value than RCTs that did not provide this type of support (P=.01; subgroup 1 IRR=0.83, 95% CI 0.72-0.95 vs subgroup 2 IRR=1.02, 95% CI 0.93-1.12). RCTs that applied mobile health were associated with a significantly lower IRR (P=.03; IRR=0.79, 95% CI 0.64-0.96 vs IRR=1.00, 95% CI 0.94-1.06) and RR (P=.01; RR=0.67, 95% CI 0.53-0.85 vs RR=0.95, 95% CI 0.84-1.07).
Conclusions: Telemonitoring strategies involving medication support and mobile health were associated with improvements in all-cause mortality or hospitalization outcomes. These strategies should be prioritized in telemonitoring interventions for the management of patients with chronic heart failure.
Keywords: chronic heart failure; meta-analysis; mobile health; systematic review; telehealth; telemonitoring.
©Hang Ding, Sheau Huey Chen, Iain Edwards, Rajiv Jayasena, James Doecke, Jamie Layland, Ian A Yang, Andrew Maiorana. Originally published in the Journal of Medical Internet Research (http://www.jmir.org), 13.11.2020.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
Similar articles
-
Which components of heart failure programmes are effective? A systematic review and meta-analysis of the outcomes of structured telephone support or telemonitoring as the primary component of chronic heart failure management in 8323 patients: Abridged Cochrane Review.Eur J Heart Fail. 2011 Sep;13(9):1028-40. doi: 10.1093/eurjhf/hfr039. Epub 2011 Jul 6. Eur J Heart Fail. 2011. PMID: 21733889
-
Effectiveness of telemedicine systems for adults with heart failure: a meta-analysis of randomized controlled trials.Heart Fail Rev. 2020 Mar;25(2):231-243. doi: 10.1007/s10741-019-09801-5. Heart Fail Rev. 2020. PMID: 31197564 Free PMC article. Review.
-
Home Telemonitoring In Heart Failure: A Systematic Review And Meta-Analysis.Health Aff (Millwood). 2018 Dec;37(12):1983-1989. doi: 10.1377/hlthaff.2018.05087. Health Aff (Millwood). 2018. PMID: 30633680
-
Comparative Effectiveness of Disease Management With Information Communication Technology for Preventing Hospitalization and Readmission in Adults With Chronic Congestive Heart Failure.J Am Med Dir Assoc. 2018 Jun;19(6):472-479. doi: 10.1016/j.jamda.2018.03.012. Epub 2018 May 3. J Am Med Dir Assoc. 2018. PMID: 29730178
-
Home telemonitoring for type 2 diabetes: an evidence-based analysis.Ont Health Technol Assess Ser. 2009;9(24):1-38. Epub 2009 Oct 1. Ont Health Technol Assess Ser. 2009. PMID: 23074529 Free PMC article.
Cited by
-
RELEASE-HF study: a protocol for an observational, registry-based study on the effectiveness of telemedicine in heart failure in the Netherlands.BMJ Open. 2024 Jan 4;14(1):e078021. doi: 10.1136/bmjopen-2023-078021. BMJ Open. 2024. PMID: 38176879 Free PMC article.
-
Wearable Cardioverter-Defibrillator Used as a Telemonitoring System in a Real-Life Heart Failure Unit Setting.J Clin Med. 2021 Nov 22;10(22):5435. doi: 10.3390/jcm10225435. J Clin Med. 2021. PMID: 34830724 Free PMC article.
-
Virtual healthcare solutions in heart failure: a literature review.Front Cardiovasc Med. 2023 Sep 7;10:1231000. doi: 10.3389/fcvm.2023.1231000. eCollection 2023. Front Cardiovasc Med. 2023. PMID: 37745104 Free PMC article. Review.
-
An evidence map of systematic reviews on models of outpatient care for patients with chronic heart diseases.Syst Rev. 2023 May 6;12(1):80. doi: 10.1186/s13643-023-02227-z. Syst Rev. 2023. PMID: 37149625 Free PMC article.
-
Use of Facial Morphology to Determine Nutritional Status in Older Adults: Opportunities and Challenges.JMIR Public Health Surveill. 2022 Jul 18;8(7):e33478. doi: 10.2196/33478. JMIR Public Health Surveill. 2022. PMID: 35849429 Free PMC article.
References
-
- Savarese G, Lund LH. Global Public Health Burden of Heart Failure. Card Fail Rev. 2017 Apr;3(1):7–11. doi: 10.15420/cfr.2016:25:2. http://europepmc.org/abstract/MED/28785469 - DOI - PMC - PubMed
-
- Burnett H, Earley A, Voors AA, Senni M, McMurray JJ, Deschaseaux C, Cope S. Thirty Years of Evidence on the Efficacy of Drug Treatments for Chronic Heart Failure With Reduced Ejection Fraction: A Network Meta-Analysis. Circ Heart Fail. 2017 Jan;10(1):e003529. doi: 10.1161/CIRCHEARTFAILURE.116.003529. http://europepmc.org/abstract/MED/28087688 - DOI - PMC - PubMed
-
- Riley JP, Masters J. Practical multidisciplinary approaches to heart failure management for improved patient outcome. Eur Heart J Suppl. 2016 Dec 06;18(suppl G):G43–G52. doi: 10.1093/eurheartj/suw046. - DOI
-
- Jeon Y, Kraus SG, Jowsey T, Glasgow NJ. The experience of living with chronic heart failure: a narrative review of qualitative studies. BMC Health Serv Res. 2010 Mar 24;10(1):77. doi: 10.1186/1472-6963-10-77. https://bmchealthservres.biomedcentral.com/articles/10.1186/1472-6963-10-77 - DOI - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
