

Does prior ultrasonography affect the safety of induced abortion at or after 13 weeks' gestation? A retrospective study
- PMID: 33185906
- PMCID: PMC8246849
- DOI: 10.1111/aogs.14040
Does prior ultrasonography affect the safety of induced abortion at or after 13 weeks' gestation? A retrospective study
Abstract
Introduction: We aimed to assess whether ultrasonography prior to dilation and evacuation or medical abortion ≥13 weeks was correlated with safety.
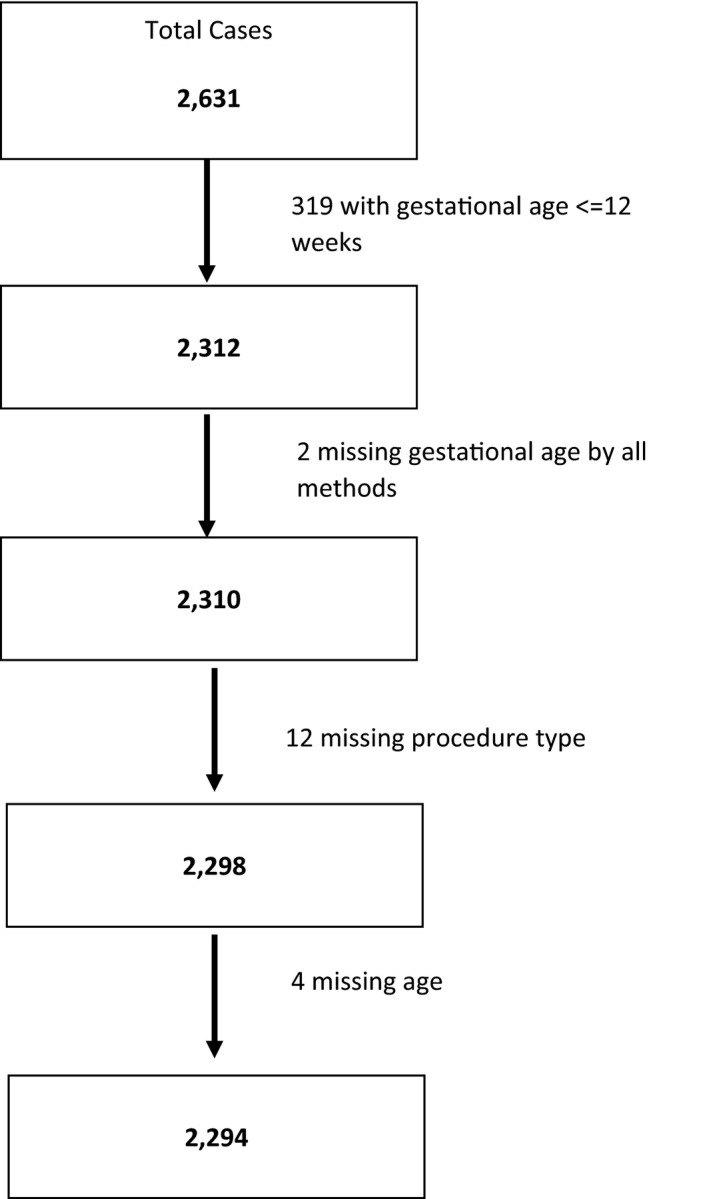
Material and methods: We conducted a retrospective chart review of patients undergoing abortion ≥13 weeks at eight sites in Nepal from 2015 to 2019.
Results: We included 2294 women undergoing abortion ≥13 weeks (no upper gestational age limit); 593 underwent dilation and evacuation and 1701 had a medical abortion. Demographics differed by procedure for parity (19% vs 33% nulliparous, dilation and evacuation, and medical abortion) and gestational age (90% vs 52% were 13-15 weeks, dilation and evacuation, and medical abortion). Ultrasonography was performed in 81% of cases overall. Complications were rare (<1% of dilations and evacuations, 1.4% of medical abortions). The most common adverse events with dilation and evacuation were hemorrhage and cervical laceration; three women required re-aspiration. Following medical abortion, 13.5% had retained products, 12.9% with prior ultrasound and 16.3% who had not had an ultrasound. Hemorrhage and severe side-effects occurred at similarly low rates regardless of whether ultrasonography was performed. In a logistic regression model where patient characteristics and case clustering within facilities were controlled for, we found a correlation between ultrasonography and complications when retained placenta was included in the model, but there was no correlation between ultrasonography and complications when retained placenta was excluded.
Conclusions: This study confirms low complication rates among women having an abortion ≥13 weeks' gestation in healthcare facilities. Settings without universal availability of ultrasound may still maintain low, comparable complication rates.
Keywords: adverse events; dilation and evacuation; medical abortion; placental retention; second trimester abortion; termination of pregnancy; ultrasonography.
© 2020 The Authors. Acta Obstetricia et Gynecologica Scandinavica published by John Wiley & Sons Ltd on behalf of Nordic Federation of Societies of Obstetrics and Gynecology (NFOG).
Conflict of interest statement
None.
References
-
- Constant D, Kluge J, Harries J, Grossman D. An analysis of delays among women accessing second‐trimester abortion in the public sector in South Africa. Contraception. 2019;100:209–213. - PubMed
-
- Baum S, DePiñeres T, Grossman D. Delays and barriers to care in Colombia among women obtaining legal first‐ and second‐trimester abortion. Int J Gynaecol Obstet. 2015;131:285–288. - PubMed
-
- Swanson M, Karasek D, Drey E, Foster DG. Delayed pregnancy testing and second‐trimester abortion: can public health interventions assist with earlier detection of unintended pregnancy? Contraception. 2014;89:400–406. - PubMed
-
- Pazol K, Creanga AA, Jamieson DJ. Abortion Surveillance – United States, 2012. MMWR Surveill Summ. 2015;64:1–40. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
