

Disease Mechanisms of Perioperative Organ Injury
- PMID: 33186161
- PMCID: PMC7673233
- DOI: 10.1213/ANE.0000000000005191
Disease Mechanisms of Perioperative Organ Injury
Abstract
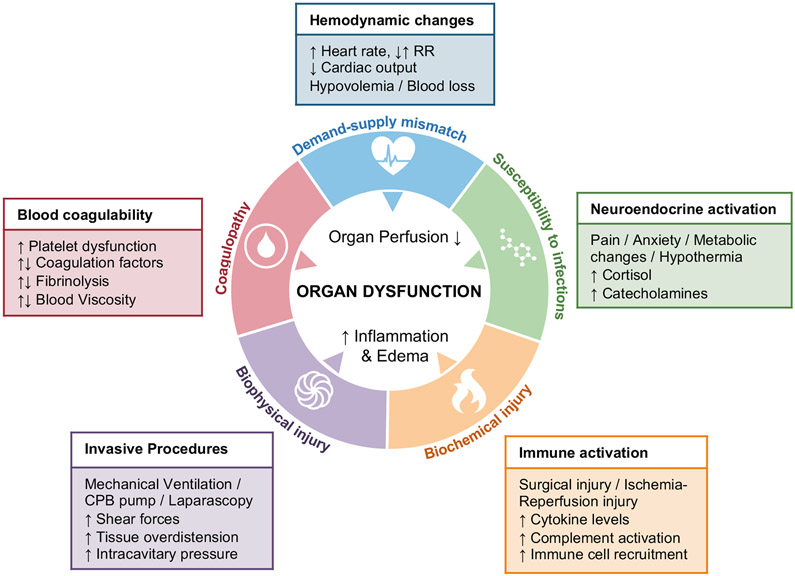
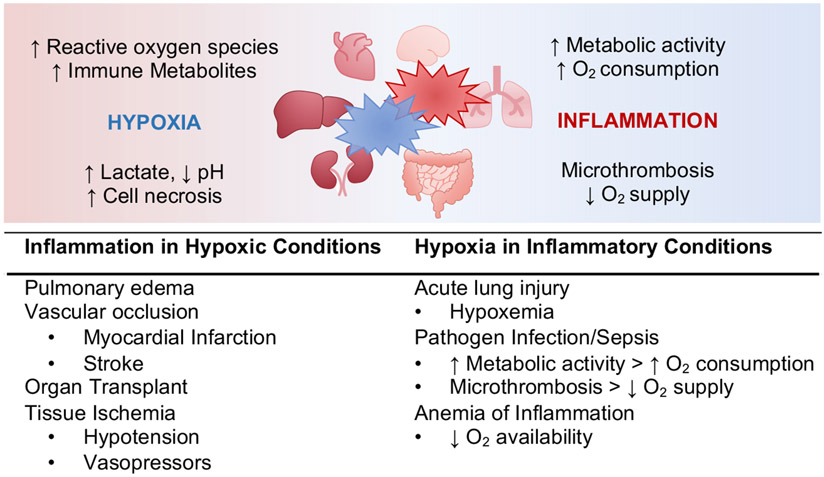
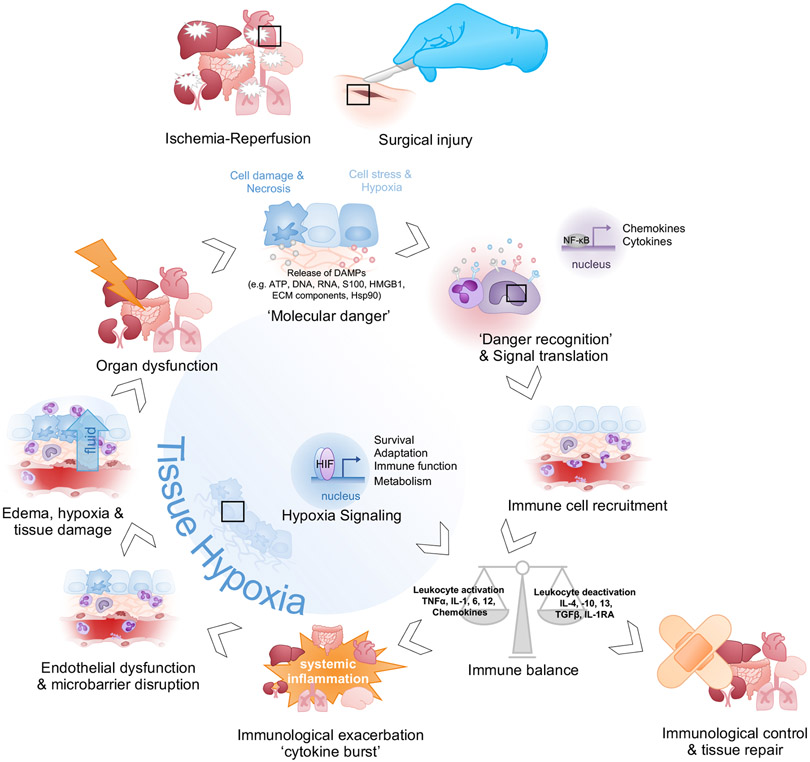
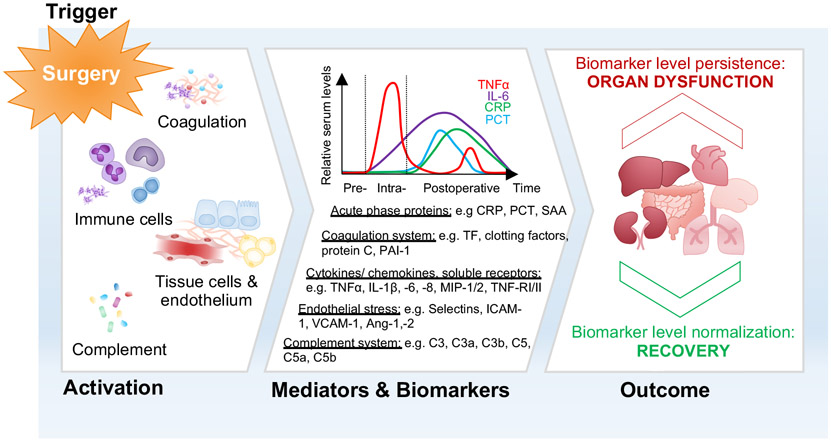
Despite substantial advances in anesthesia safety within the past decades, perioperative mortality remains a prevalent problem and can be considered among the top causes of death worldwide. Acute organ failure is a major risk factor of morbidity and mortality in surgical patients and develops primarily as a consequence of a dysregulated inflammatory response and insufficient tissue perfusion. Neurological dysfunction, myocardial ischemia, acute kidney injury, respiratory failure, intestinal dysfunction, and hepatic impairment are among the most serious complications impacting patient outcome and recovery. Pre-, intra-, and postoperative arrangements, such as enhanced recovery after surgery programs, can contribute to lowering the occurrence of organ dysfunction, and mortality rates have improved with the advent of specialized intensive care units and advances in procedures relating to extracorporeal organ support. However, no specific pharmacological therapies have proven effective in the prevention or reversal of perioperative organ injury. Therefore, understanding the underlying mechanisms of organ dysfunction is essential to identify novel treatment strategies to improve perioperative care and outcomes for surgical patients. This review focuses on recent knowledge of pathophysiological and molecular pathways leading to perioperative organ injury. Additionally, we highlight potential therapeutic targets relevant to the network of events that occur in clinical settings with organ failure.
Conflict of interest statement
Figures
Comment in
-
Perioperative Organ Failure: A Preventable Complication?Anesth Analg. 2020 Dec;131(6):1663-1665. doi: 10.1213/ANE.0000000000005244. Anesth Analg. 2020. PMID: 33186154 No abstract available.
References
-
- Haynes AB, Weiser TG, Berry WR, et al. A surgical safety checklist to reduce morbidity and mortality in a global population. N Engl J Med. 2009;360(5):491–499. - PubMed
-
- Glance LG, Lustik SJ, Hannan EL, et al. The Surgical Mortality Probability Model: derivation and validation of a simple risk prediction rule for noncardiac surgery. Ann Surg. 2012;255(4):696–702. - PubMed
-
- Nepogodiev D, Martin J, Biccard B, Makupe A, Bhangu A, Surgery NIfHRGHRUoG. Global burden of postoperative death. Lancet. 2019;393(10170):401. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
