

On the importance of the hip abductors during a clinical one legged balance test: A theoretical study
- PMID: 33186397
- PMCID: PMC7665826
- DOI: 10.1371/journal.pone.0242454
On the importance of the hip abductors during a clinical one legged balance test: A theoretical study
Abstract
Background: The ability to balance on one foot for a certain time is a widely used clinical test to assess the effects of age and diseases like peripheral neuropathy on balance. While state-space methods have been used to explore the mechanical demands and achievable accelerations for balancing on two feet in the sagittal plane, less is known about the requirements for sustaining one legged balance (OLB) in the frontal plane.
Research question: While most studies have focused on ankle function in OLB, can age and/or disease-related decreases in maximum hip abduction strength also affect OLB ability?
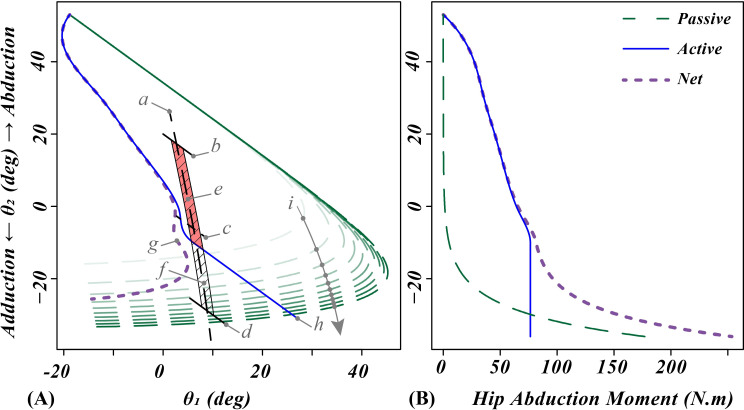
Methods: A two-link frontal plane state space model was used to define and explore the 'feasible balance region' which helps reveal the requirements for maintaining and restoring OLB, given the adverse effects of age and peripheral neuropathy on maximum hip and ankle strengths.
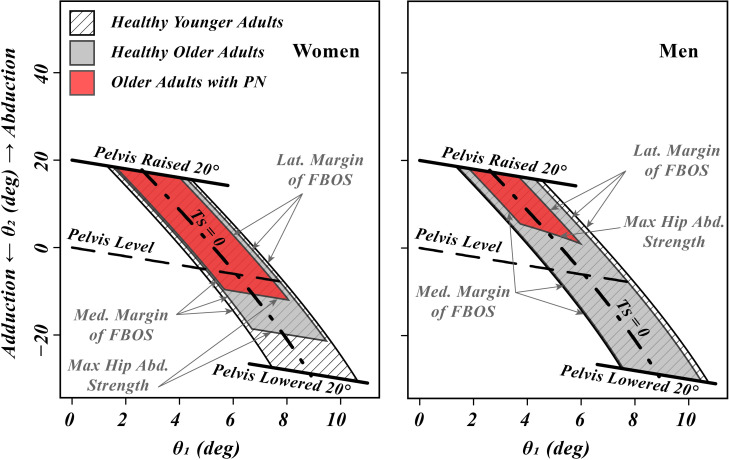
Results: Maintaining quasistatic OLB required 50%-106% of the maximum hip abduction strength in young and older adults, and older patients with peripheral neuropathy. Effectiveness of a 'hip strategy' in recovering OLB was heavily dependent on the maximum hip abduction strength, and for healthy older women was as important as ankle strength. Natural reductions of strength due to healthy aging did not show a meaningful reduction in meeting the strength requirement of clinical OLB. However deficits in hip strength typical of patients with peripheral neuropathy did adversely affect both quasistatic OLB and recoverable OLB states.
Significance: The importance of hip muscle strength has been underappreciated in the clinical OLB test. This is partly because the passive tissues of the hip joint can mask moderate deficits in hip abduction strength until it is needed for recovering OLB. Adding a follow up OLB test with a slightly raised pelvis would be a simple way to check for adequate hip abductor muscle strength.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures



References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
