

The Association of Orthostatic Hypotension With Ambulatory Blood Pressure Phenotypes in SPRINT
- PMID: 33186448
- PMCID: PMC8140655
- DOI: 10.1093/ajh/hpaa184
The Association of Orthostatic Hypotension With Ambulatory Blood Pressure Phenotypes in SPRINT
Abstract
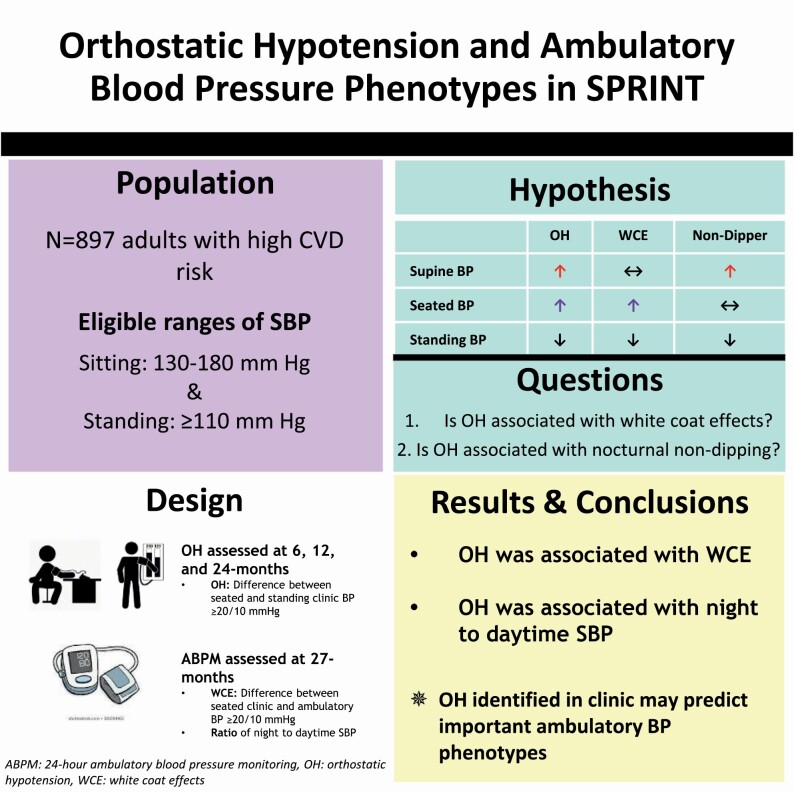
Background: Clinic blood pressure (BP) when measured in the seated position, can miss meaningful BP phenotypes, including low ambulatory BP (white coat effects [WCE]) or high supine BP (nocturnal non-dipping). Orthostatic hypotension (OH) measured using both seated (or supine) and standing BP, could identify phenotypes poorly captured by seated clinic BP alone.
Methods: We examined the association of OH with WCE and night-to-daytime systolic BP (SBP) in a subpopulation of SPRINT, a randomized trial testing the effects of intensive or standard (<120 vs. <140 mm Hg) SBP treatment strategies in adults at increased risk of cardiovascular disease. OH was assessed during follow-up (6, 12, and 24 months) and defined as a decrease in mean seated SBP ≥20 or diastolic BP ≥10 mm Hg after 1 min of standing. WCE, based on 24-hour ambulatory BP monitoring performed at 27 months, was defined as the difference between 27-month seated clinic and daytime ambulatory BP ≥20/≥10 mm Hg. Reverse dipping was defined as a ratio of night-to-daytime SBP >1.
Results: Of 897 adults (mean age 71.5±9.5 years, 29% female, 28% black), 128 had OH at least once. Among those with OH, 15% had WCE (vs. 7% without OH). Moreover, 25% of those with OH demonstrated a non-dipping pattern (vs. 14% without OH). OH was positively associated with both WCE (OR=2.24; 95%CI: 1.28, 4.27) and reverse dipping (OR=2.29; 95% CI: 1.31, 3.99).
Conclusions: The identification of OH in clinic was associated with two BP phenotypes often missed with traditional seated BP assessments. Further studies on mechanisms of these relationships are needed.
Clinical trials registration: Trial Number NCT03569020.
Keywords: ambulatory blood pressure monitoring; blood pressure; hypertension; nocturnal dipping status; orthostatic hypotension; white coat effects.
© American Journal of Hypertension, Ltd 2020. All rights reserved. For Permissions, please email: journals.permissions@oup.com.
References
-
- Whelton PK, Carey RM, Aronow WS, Casey DE Jr, Collins KJ, Dennison Himmelfarb C, DePalma SM, Gidding S, Jamerson KA, Jones DW, MacLaughlin EJ, Muntner P, Ovbiagele B, Smith SC Jr, Spencer CC, Stafford RS, Taler SJ, Thomas RJ, Williams KA Sr, Williamson JD, Wright JT Jr. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension 2018; 71:e13–e115. - PubMed
-
- Ghazi L, Pajewski NM, Rifkin DE, Bates JT, Chang TI, Cushman WC, Glasser SP, Haley WE, Johnson KC, Kostis WJ, Papademetriou V, Rahman M, Simmons DL, Taylor A, Whelton PK, Wright JT, Bhatt UY, Drawz PE. Effect of intensive and standard clinic-based hypertension management on the concordance between clinic and ambulatory blood pressure and blood pressure variability in SPRINT. J Am Heart Assoc 2019; 8:e011706. - PMC - PubMed
-
- Wright JT Jr, Williamson JD, Whelton PK, Snyder JK, Sink KM, Rocco MV, Reboussin DM, Rahman M, Oparil S, Lewis CE, Kimmel PL, Johnson KC, Goff DC Jr, Fine LJ, Cutler JA, Cushman WC, Cheung AK, Ambrosius WT; SPRINT Research Group . A randomized trial of intensive versus standard blood-pressure control. N Engl J Med 2015; 373:2103–2116. - PMC - PubMed
-
- Kaufmann H. Consensus statement on the definition of orthostatic hypotension, pure autonomic failure and multiple system atrophy. Clin Auton Res 1996; 6:125–126. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
