

Longitudinal assessment of racial disparities in juvenile idiopathic arthritis disease activity in a treat-to-target intervention
- PMID: 33187519
- PMCID: PMC7666526
- DOI: 10.1186/s12969-020-00485-y
Longitudinal assessment of racial disparities in juvenile idiopathic arthritis disease activity in a treat-to-target intervention
Abstract
Background: We sought to evaluate racial disparities in disease outcomes among children with polyarticular juvenile idiopathic arthritis (JIA) during a treat-to-target (TTT) intervention with clinical decision support (CDS).
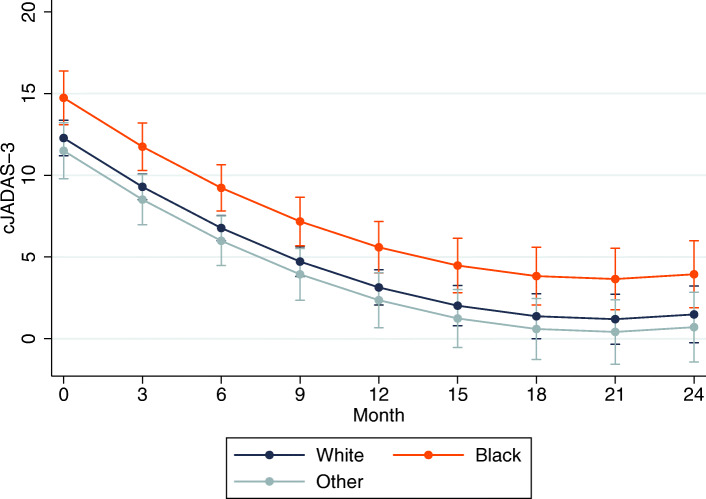
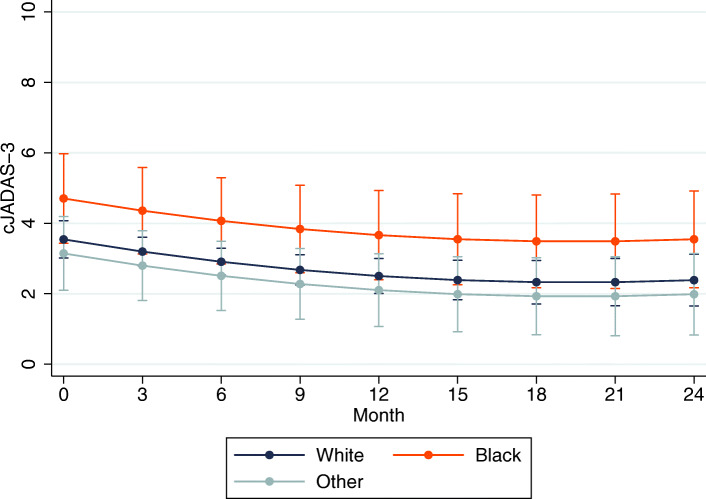
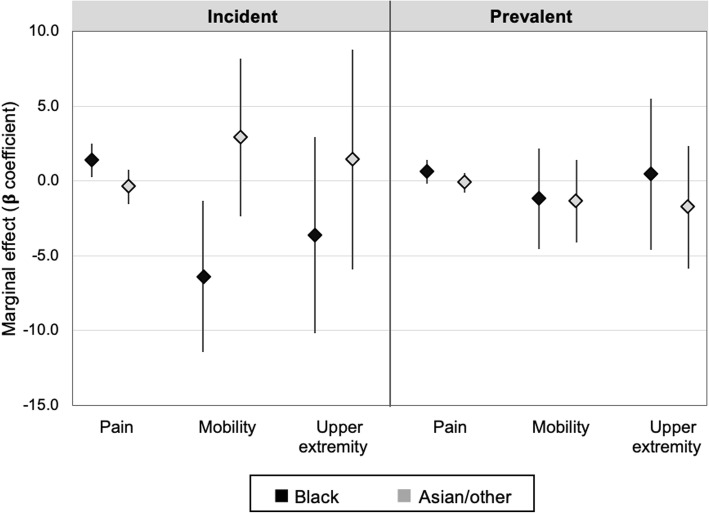
Methods: This was a retrospective analysis of a TTT-CDS strategy integrated into clinical practice for children with polyarticular JIA at a single center from 2016 to 2019. The primary outcome was the clinical Juvenile Arthritis Disease Activity Score (cJADAS-10). We used multivariable linear regression to assess racial differences in disease outcomes at the index visit (first visit after implementation). The effect of race on disease outcomes over time was estimated using linear mixed-effects models, stratified by incident or prevalent disease.
Results: We included 159 children with polyarticular JIA, of which 74, 13 and 13% were white, black, and Asian/other, respectively. cJADAS-10 improved significantly over time for all race categories, while the rates of improvement did not differ by race in incident (p = 0.53) or prevalent cases (p = 0.58). cJADAS-10 over time remained higher among black children compared to white children (β 2.5, p < 0.01 and β 1.2, p = 0.08 for incident and prevalent cases, respectively). Provider attestation to CDS use at ≥50% of encounters was associated with a 3.9 greater reduction in cJADAS-10 among black children compared to white children (p = 0.02).
Conclusion: Despite similar rates of improvement over time by race, disparities in JIA outcomes persisted throughout implementation of a TTT-CDS approach. More consistent CDS use may have a greater benefit among black children and needs to be explored further.
Keywords: Healthcare disparities; Juvenile arthritis; Patient outcome assessment; Patient reported outcome measures; Pediatrics.
Conflict of interest statement
J.C. and J.B. report grant funding from GlaxoSmithKline for research outside of this work. The remaining listed authors declare they have no competing interests.
Figures
References
-
- Ringold S, Beukelman T, Nigrovic PA, Kimura Y. CARRA registry site principal investigators, Birmingham J, et al. race, ethnicity, and disease outcomes in juvenile idiopathic arthritis: a cross-sectional analysis of the childhood arthritis and rheumatology research Alliance (CARRA) registry. J Rheumatol. 2013;40(6):936–942. doi: 10.3899/jrheum.121147. - DOI - PubMed
-
- Bruce B, Fries JF, Murtagh KN. Health status disparities in ethnic minority patients with rheumatoid arthritis: a cross-sectional study. J Rheumatol. 2007;34(7):1475–1479. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
