

When hematologic malignancies meet COVID-19 in the United States: Infections, death and disparities
- PMID: 33187811
- PMCID: PMC7833659
- DOI: 10.1016/j.blre.2020.100775
When hematologic malignancies meet COVID-19 in the United States: Infections, death and disparities
Abstract
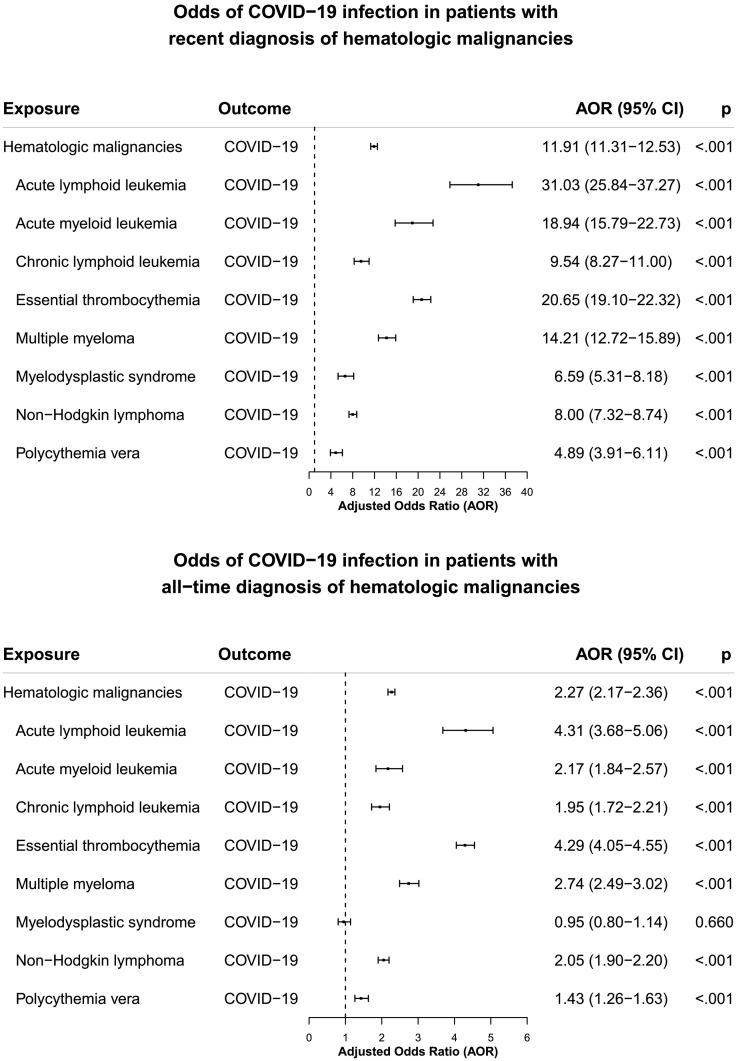
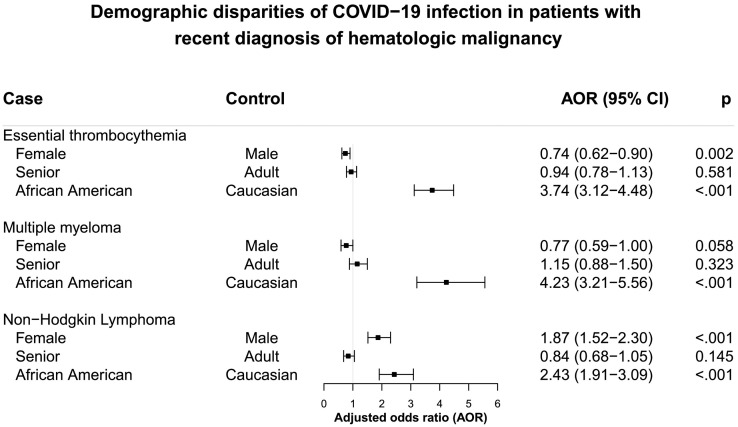
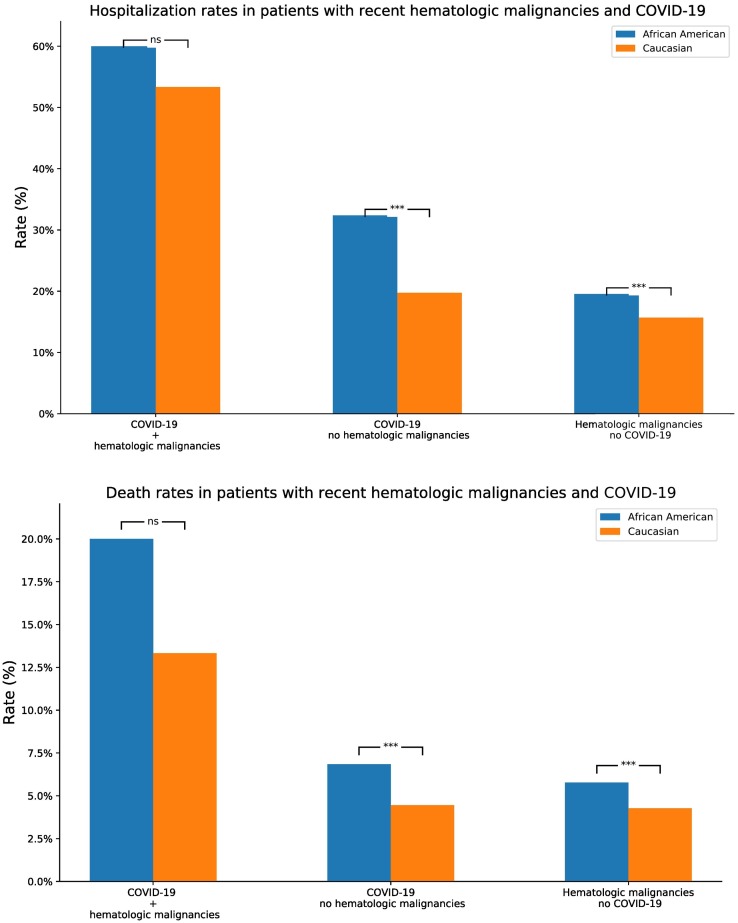
Scientific data is limited on the risks, adverse outcomes and racial disparities for COVID-19 illness in individuals with hematologic malignancies in the United States. To fill this void, we screened and analyzed a nation-wide database of patient electronic health records (EHRs) of 73 million patients in the US (up to September 1st) for COVID-19 and eight major types of hematologic malignancies. Patients with hematologic malignancies had increased odds of COVID-19 infection compared with patients without hematologic malignancies for both all-time diagnosis (malignancy diagnosed in the past year or prior) (adjusted Odds ratio or AOR: 2.27 [2.17-2.36], p < 0.001) and recent diagnosis (malignancy diagnosed in the past year) (AOR:11.91 [11.31-12.53], p < 0.001), with strongest effect for recently diagnosed acute lymphoid leukemia (AOR: 31.03 [25.87-37.27], p < 0.001), essential thrombocythemia (AOR: 20.65 [19.10-22.32], p < 0.001), acute myeloid leukemia (AOR: 18.94 [15.79-22.73], p < 0.001), multiple myeloma (AOR: 14.21 [12.72-15.89], p < 0.001). Among patients with hematologic malignancies, African Americans had higher odds of COVID-19 infection than Caucasians with largest racial disparity for multiple myeloma (AOR: 4.23 [3.21-5.56], p < 0.001). Patients with recently diagnosed hematologic malignancies had worse outcomes (hospitalization: 51.9%, death: 14.8%) than COVID-19 patients without hematologic malignancies (hospitalization: 23.5%, death: 5.1%) (p < 0.001) and hematologic malignancy patients without COVID-19 (hospitalization: 15.0%, death: 4.1%) (p < 0.001).
Keywords: COVID-19; Disparity; Health outcomes; Hematologic malignancies; Risk.
Copyright © 2020 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Q.W., N.A.B, and R.X have no financial interests to disclose.
Figures
References
-
- CDC Cases in the U.S. https://www.cdc.gov/coronavirus/2019-ncov/cases-updates/cases-in-us.html (accessed on September 1st, 2020)
-
- CDC Groups at Higher Risk for COVID-19 Severe Illness. https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/groups-... (accessed on June 28, 2020)
-
- Richardson S., Hirsch J.S., Narasimhan M., Crawford J.M., McGinn T., Davidson K.W. Presenting characteristics, comorbidities, and outcomes among 5700 patients hospitalized with COVID-19 in the new York City area [published correction appears in doi: 10.1001/jama.2020.7681] JAMA. 2020;323(20):2052–2059. doi: 10.1001/jama.2020.6775. - DOI - PMC - PubMed
-
- Zhou F., Yu T., Du R., Fan G., Liu Y., Liu Z. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020 Mar 28;395(10229):1054–1062. doi: 10.1016/S0140-6736(20)30566-3. [Erratum in Lancet. 2020 Mar 28;395(10229):1038. doi: 10.1016/S0140-6736(20)30606-1. Epub 2020 Mar 12. PMID: 32171424] [Erratum in Lancet. 2020 Mar 28;395(10229):1038. doi: 10.1016/S0140-6736(20)30638-3. Epub 2020 Mar 17. PMID: 32192581] - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
