

Outcomes for Out-of-Hospital Cardiac Arrest in the United States During the Coronavirus Disease 2019 Pandemic
- PMID: 33188678
- PMCID: PMC7666759
- DOI: 10.1001/jamacardio.2020.6210
Outcomes for Out-of-Hospital Cardiac Arrest in the United States During the Coronavirus Disease 2019 Pandemic
Abstract
Importance: Recent reports from communities severely affected by the coronavirus disease 2019 (COVID-19) pandemic found lower rates of sustained return of spontaneous circulation (ROSC) for out-of-hospital cardiac arrest (OHCA). Whether the pandemic has affected OHCA outcomes more broadly is unknown.
Objective: To assess the association between the COVID-19 pandemic and OHCA outcomes, including in areas with low and moderate COVID-19 disease burden.
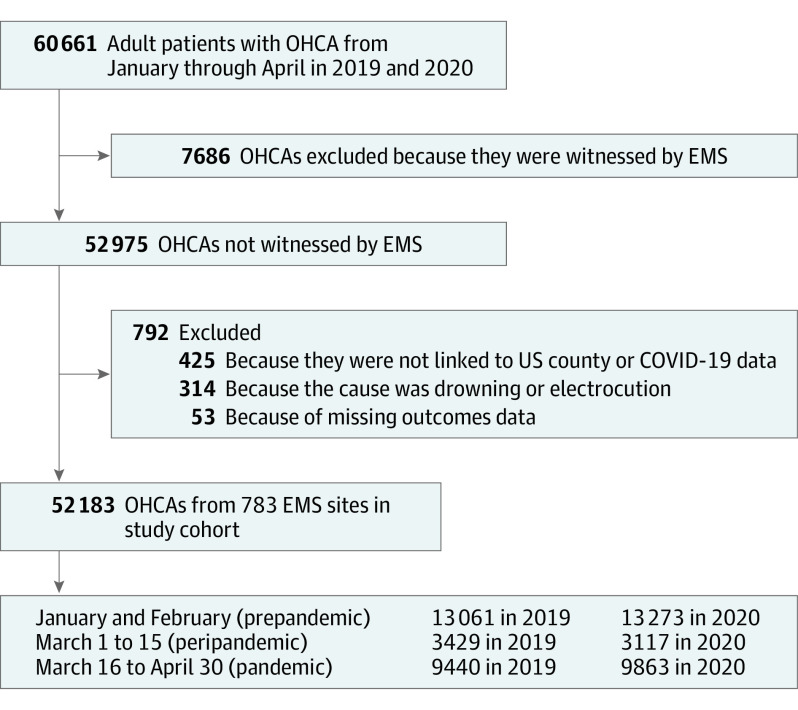
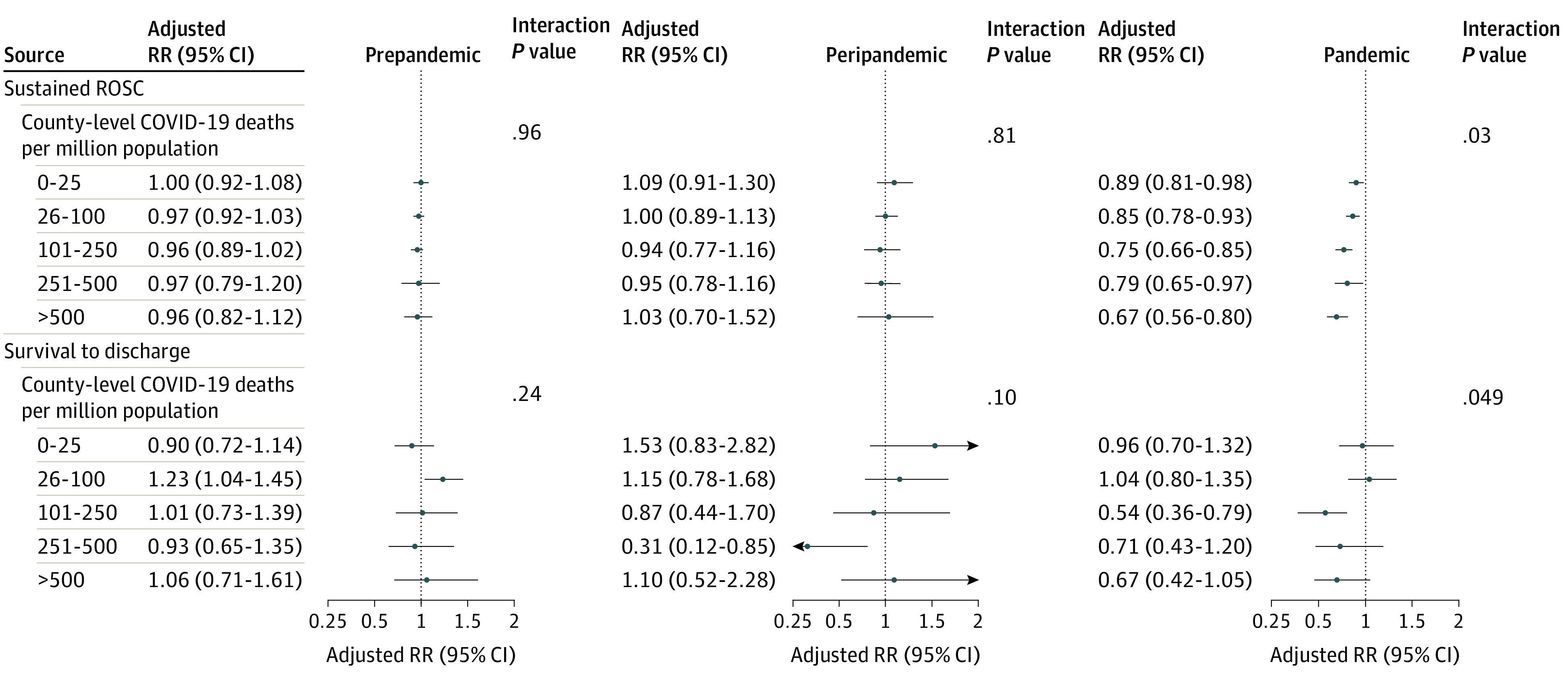
Design, setting, and participants: This study used a large US registry of OHCAs to compare outcomes during the pandemic period of March 16 through April 30, 2020, with those from March 16 through April 30, 2019. Cases were geocoded to US counties, and the COVID-19 mortality rate in each county was categorized as very low (0-25 per million residents), low (26-100 per million residents), moderate (101-250 per million residents), high (251-500 per million residents), or very high (>500 per million residents). As additional controls, the study compared OHCA outcomes during the prepandemic period (January through February) and peripandemic period (March 1 through 15).
Exposure: The COVID-19 pandemic.
Main outcomes and measures: Sustained ROSC (≥20 minutes), survival to discharge, and OHCA incidence.
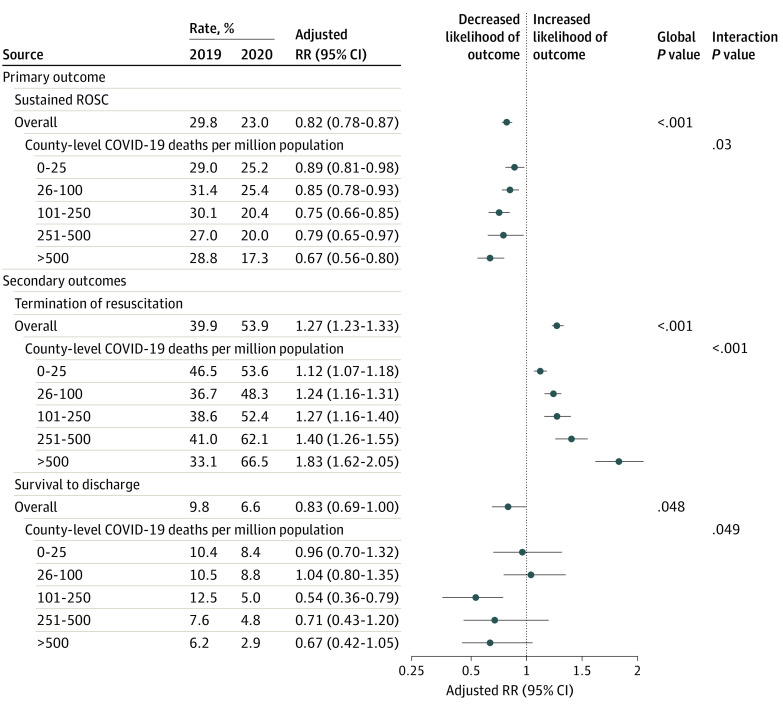
Results: A total of 19 303 OHCAs occurred from March 16 through April 30 in both years, with 9863 cases in 2020 (mean [SD] age, 62.6 [19.3] years; 6040 men [61.3%]) and 9440 in 2019 (mean [SD] age, 62.2 [19.2] years; 5922 men [62.7%]). During the pandemic, rates of sustained ROSC were lower than in 2019 (23.0% vs 29.8%; adjusted rate ratio, 0.82 [95% CI, 0.78-0.87]; P < .001). Sustained ROSC rates were lower by between 21% (286 of 1429 [20.0%] in 2020 vs 305 of 1130 [27.0%] in 2019; adjusted RR, 0.79 [95% CI, 0.65-0.97]) and 33% (149 of 863 [17.3%] in 2020 vs 192 of 667 [28.8%] in 2019; adjusted RR, 0.67 [95% CI, 0.56-0.80]) in communities with high or very high COVID-19 mortality, respectively; however, rates of sustained ROSC were also lower by 11% (583 of 2317 [25.2%] in 2020 vs 740 of 2549 [29.0%] in 2019; adjusted RR, 0.89 [95% CI, 0.81-0.98]) to 15% (889 of 3495 [25.4%] in 2020 vs 1109 of 3532 [31.4%] in 2019; adjusted RR, 0.85 [95% CI, 0.78-0.93]) in communities with very low and low COVID-19 mortality. Among emergency medical services agencies with complete data on hospital survival (7085 total patients), survival to discharge was lower during the pandemic compared with 2019 (6.6% vs 9.8%; adjusted RR, 0.83 [95% CI, 0.69-1.00]; P = .048), primarily in communities with moderate to very high COVID-19 mortality (interaction P = .049). Incidence of OHCA was higher than in 2019, but the increase was largely observed in communities with high COVID-19 mortality (adjusted mean difference, 38.6 [95% CI, 37.1-40.1] per million residents) and very high COVID-19 mortality (adjusted mean difference, 28.7 [95% CI, 26.7-30.6] per million residents). In contrast, there was no difference in rates of sustained ROSC or survival to discharge during the prepandemic and peripandemic periods in 2020 vs 2019.
Conclusions and relevance: Early during the pandemic, rates of sustained ROSC for OHCA were lower throughout the US, even in communities with low COVID-19 mortality rates. Overall survival was lower, primarily in communities with moderate or high COVID-19 mortality.
Conflict of interest statement
Figures
References
-
- McNally B, Robb R, Mehta M, et al. . Out-of-hospital cardiac arrest surveillance—Cardiac Arrest Registry to Enhance Survival (CARES), United States, October 1, 2005–December 31, 2010. MMWR Surveill Summ. 2011;60:1-19. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
