Investigating the clinico-anatomical dissociation in the behavioral variant of Alzheimer disease
- PMID: 33189136
- PMCID: PMC7666520
- DOI: 10.1186/s13195-020-00717-z
Investigating the clinico-anatomical dissociation in the behavioral variant of Alzheimer disease
Abstract
Background: We previously found temporoparietal-predominant atrophy patterns in the behavioral variant of Alzheimer's disease (bvAD), with relative sparing of frontal regions. Here, we aimed to understand the clinico-anatomical dissociation in bvAD based on alternative neuroimaging markers.
Methods: We retrospectively included 150 participants, including 29 bvAD, 28 "typical" amnestic-predominant AD (tAD), 28 behavioral variant of frontotemporal dementia (bvFTD), and 65 cognitively normal participants. Patients with bvAD were compared with other diagnostic groups on glucose metabolism and metabolic connectivity measured by [18F]FDG-PET, and on subcortical gray matter and white matter hyperintensity (WMH) volumes measured by MRI. A receiver-operating-characteristic-analysis was performed to determine the neuroimaging measures with highest diagnostic accuracy.
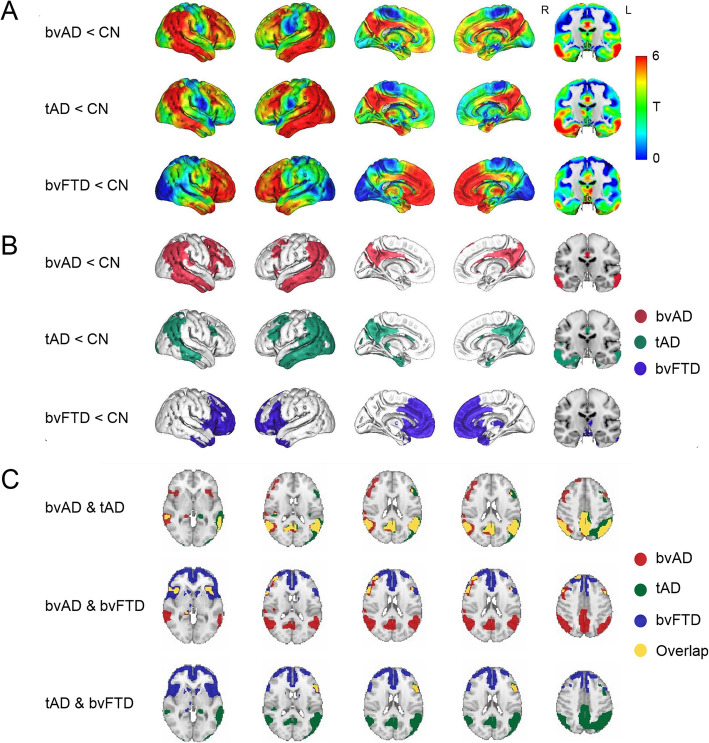
Results: bvAD and tAD showed predominant temporoparietal hypometabolism compared to controls, and did not differ in direct contrasts. However, overlaying statistical maps from contrasts between patients and controls revealed broader frontoinsular hypometabolism in bvAD than tAD, partially overlapping with bvFTD. bvAD showed greater anterior default mode network (DMN) involvement than tAD, mimicking bvFTD, and reduced connectivity of the posterior cingulate cortex with prefrontal regions. Analyses of WMH and subcortical volume showed closer resemblance of bvAD to tAD than to bvFTD, and larger amygdalar volumes in bvAD than tAD respectively. The top-3 discriminators for bvAD vs. bvFTD were FDG posterior-DMN-ratios (bvAD<bvFTD), MRI posterior-DMN-ratios (bvAD<bvFTD), MRI salience-network-ratios (bvAD>bvFTD, area under the curve [AUC] range 0.85-0.91, all p < 0.001). The top-3 for bvAD vs. tAD were amygdalar volume (bvAD>tAD), MRI anterior-DMN-ratios (bvAD<tAD), FDG anterior-DMN-ratios (bvAD<tAD, AUC range 0.71-0.84, all p < 0.05).
Conclusions: Subtle frontoinsular hypometabolism and anterior DMN involvement may underlie the prominent behavioral phenotype in bvAD.
Keywords: Alzheimer’s disease; Behavior; Frontotemporal dementia; MRI; PET.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures