

Limitations of Conventional Magnetic Resonance Imaging as a Predictor of Death or Disability Following Neonatal Hypoxic-Ischemic Encephalopathy in the Late Hypothermia Trial
- PMID: 33189747
- PMCID: PMC7914162
- DOI: 10.1016/j.jpeds.2020.11.015
Limitations of Conventional Magnetic Resonance Imaging as a Predictor of Death or Disability Following Neonatal Hypoxic-Ischemic Encephalopathy in the Late Hypothermia Trial
Abstract
Objective: To investigate if magnetic resonance imaging (MRI) is an accurate predictor for death or moderate-severe disability at 18-22 months of age among infants with neonatal encephalopathy in a trial of cooling initiated at 6-24 hours.
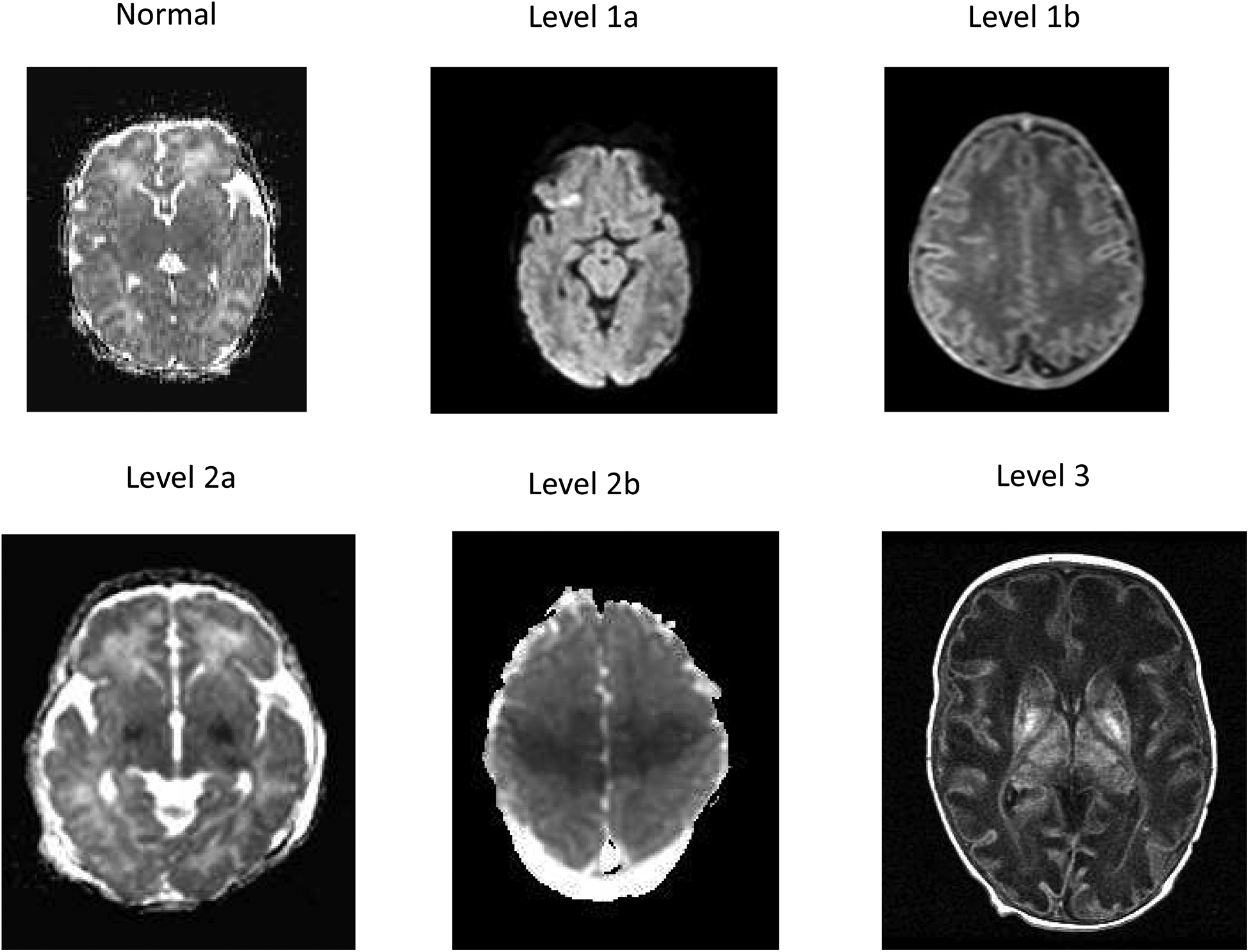
Study design: Subgroup analysis of infants ≥36 weeks of gestation with moderate-severe neonatal encephalopathy randomized at 6-24 postnatal hours to hypothermia or usual care in a multicenter trial of late hypothermia. MRI scans were performed per each center's practice and interpreted by 2 central readers using the Eunice Kennedy Shriver National Institute of Child Health and Human Development injury score (6 levels, normal to hemispheric devastation). Neurodevelopmental outcomes were assessed at 18-22 months of age.
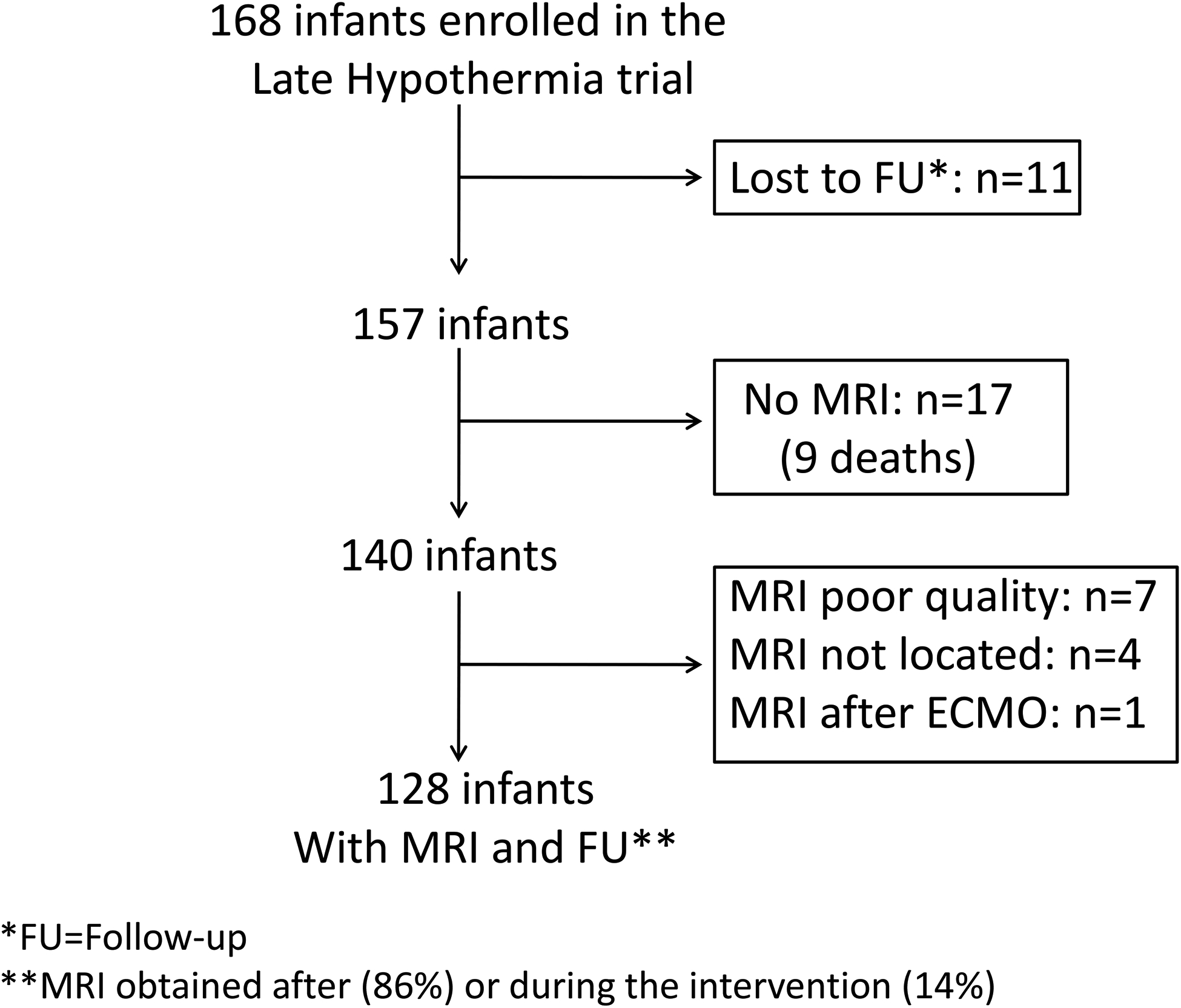
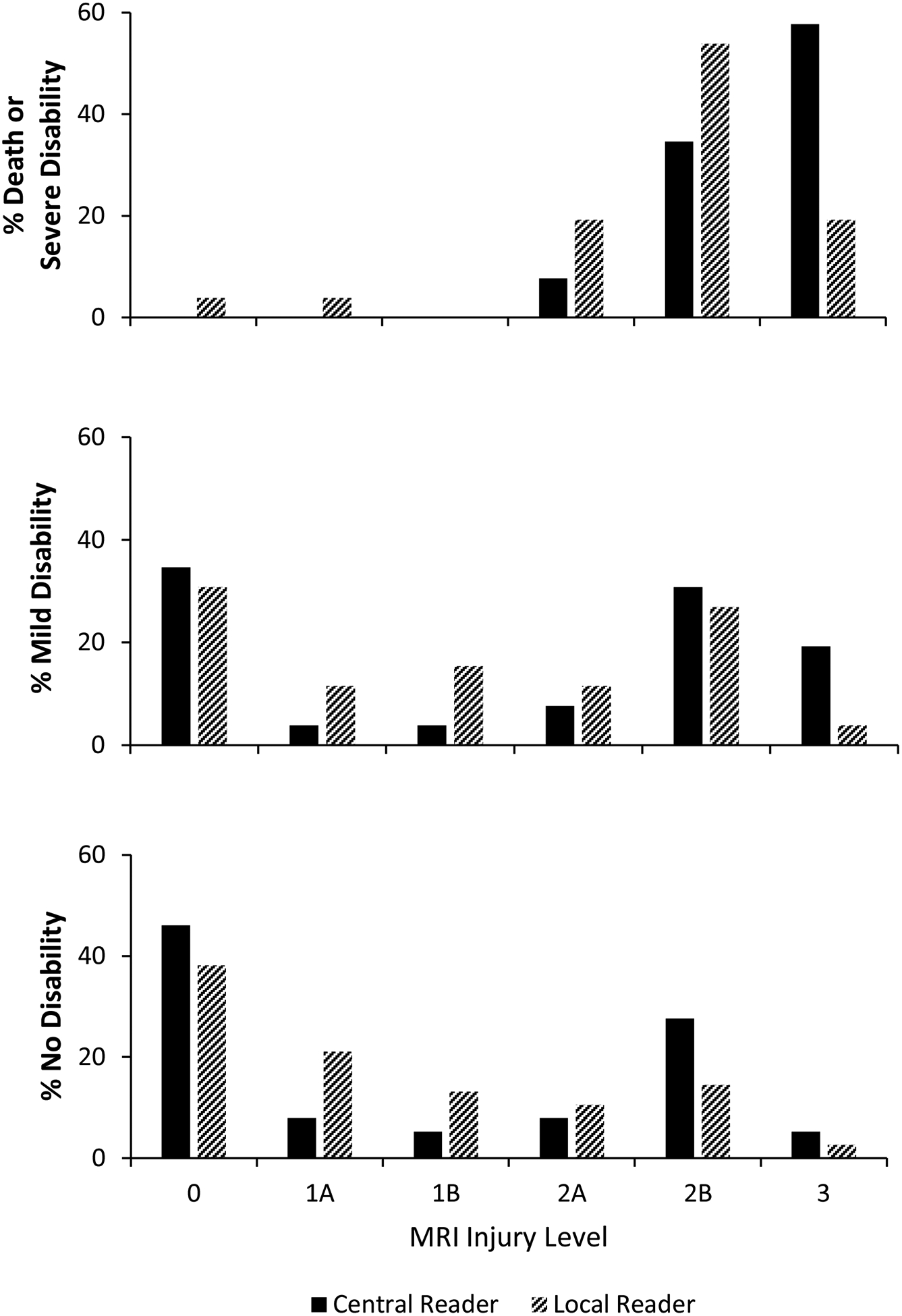
Results: Of 168 enrollees, 128 had an interpretable MRI and were seen in follow-up (n = 119) or died (n = 9). MRI findings were predominantly acute injury and did not differ by cooling treatment. At 18-22 months, death or severe disability occurred in 20.3%. No infant had moderate disability. Agreement between central readers was moderate (weighted kappa 0.56, 95% CI 0.45-0.67). The adjusted odds of death or severe disability increased 3.7-fold (95% CI 1.8-7.9) for each increment of injury score. The area under the curve for severe MRI patterns to predict death or severe disability was 0.77 and the positive and negative predictive values were 36% and 100%, respectively.
Conclusions: MRI injury scores were associated with neurodevelopmental outcome at 18-22 months among infants in the Late Hypothermia Trial. However, the results suggest caution when using qualitative interpretations of MRI images to provide prognostic information to families following perinatal hypoxia-ischemia.
Trial registration: Clinicaltrials.gov: NCT00614744.
Keywords: brain cooling; hypoxic-ischemic encephalopathy; imaging.
Copyright © 2020 Elsevier Inc. All rights reserved.
Conflict of interest statement
The National Institutes of Health, the
Figures
References
-
- American College of Obstetricians and Gynecologists, American Academy of Pediatrics. Neonatal Encephalopathy and Neurologic Outcome, 2nd Ed. Washington, DC: American College of Obstetricians and Gynecologists; 2014.
-
- Miller SP, Ramaswamy V, Michelson D, Barkovich AJ, Holshouser B, Wycliffe N, et al. Patterns of brain injury in term neonatal encephalopathy. J Pediatr. 2005;146:453–60. - PubMed
-
- Myers RE. Two patterns of perinatal brain damage and their conditions of occurrence. Am J Obstet Gynecol. 1972;112:246–76. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
