

Intestinal Dysbiosis Amplifies Acetaminophen-Induced Acute Liver Injury
- PMID: 33189892
- PMCID: PMC7900526
- DOI: 10.1016/j.jcmgh.2020.11.002
Intestinal Dysbiosis Amplifies Acetaminophen-Induced Acute Liver Injury
Abstract
Background & aims: Acute liver failure (ALF) represents an unmet medical need in Western countries. Although the link between intestinal dysbiosis and chronic liver disease is well-established, there is little evidence for a functional role of gut-liver interaction during ALF. Here we hypothesized that intestinal dysbiosis may affect ALF.
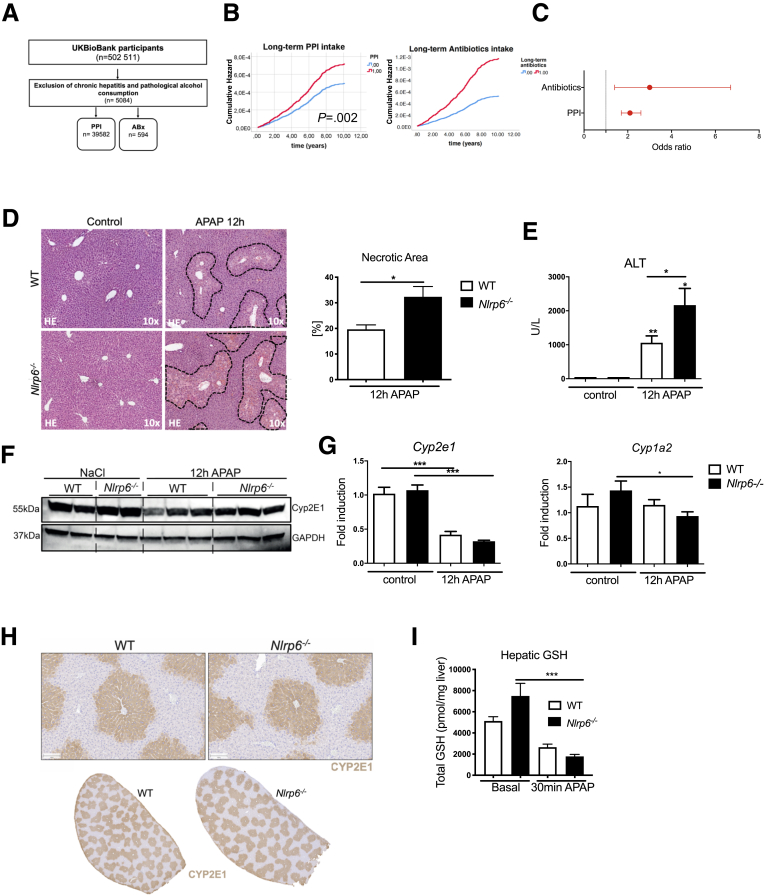
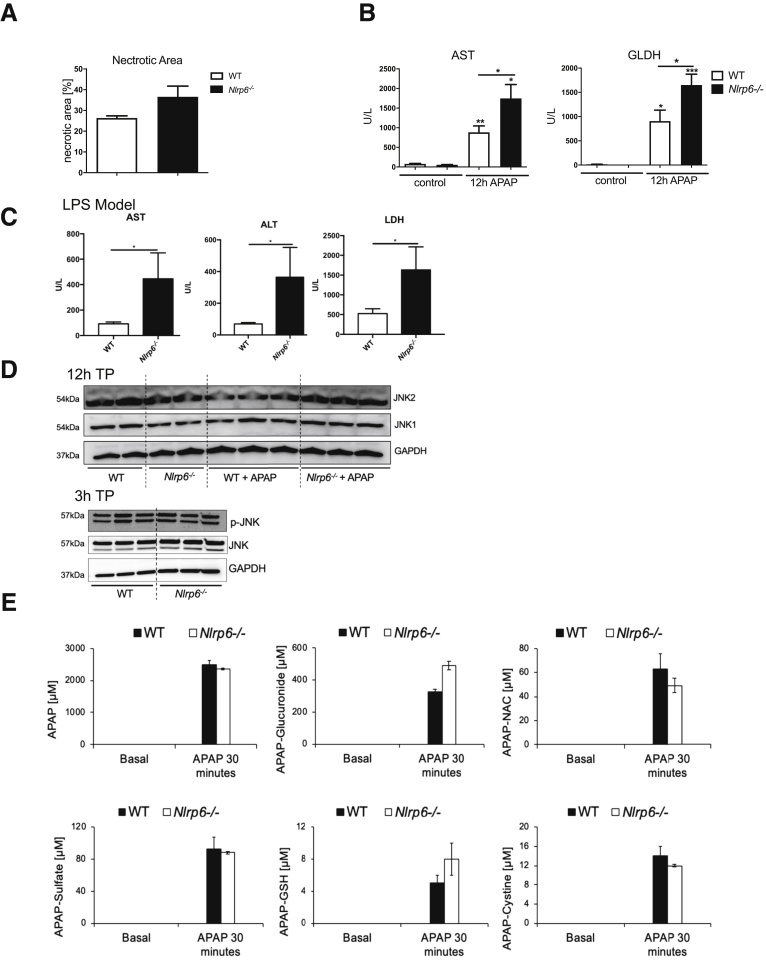
Methods: To test this hypothesis, we assessed the association of proton pump inhibitor (PPI) or long-term antibiotics (ABx) intake, which have both been linked to intestinal dysbiosis, and occurrence of ALF in the 500,000 participants of the UK BioBank population-based cohort. For functional studies, male Nlrp6-/- mice were used as a dysbiotic mouse model and injected with a sublethal dose of acetaminophen (APAP) or lipopolysaccharide (LPS) to induce ALF.
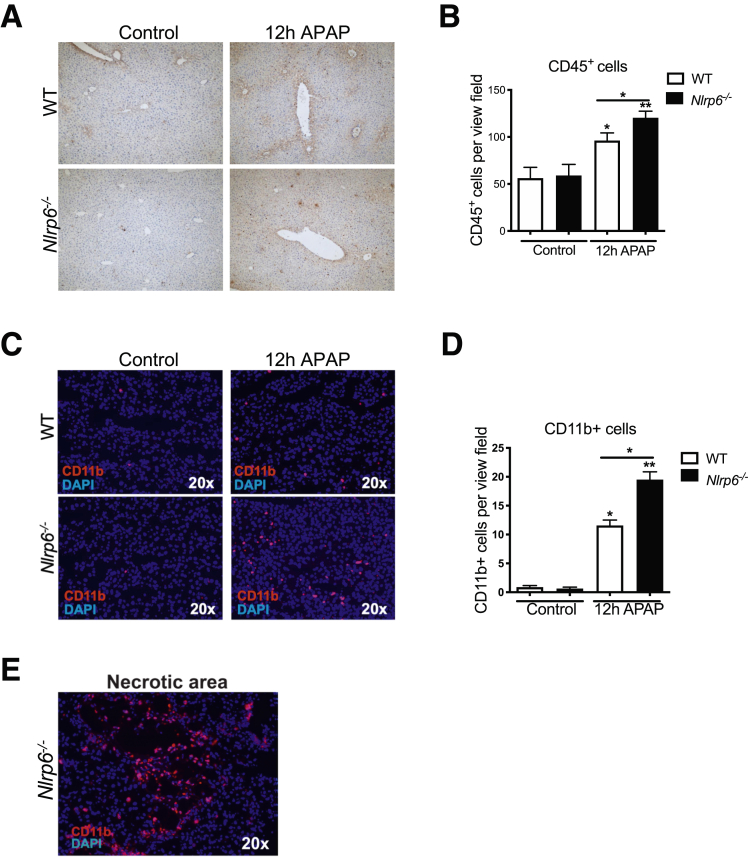
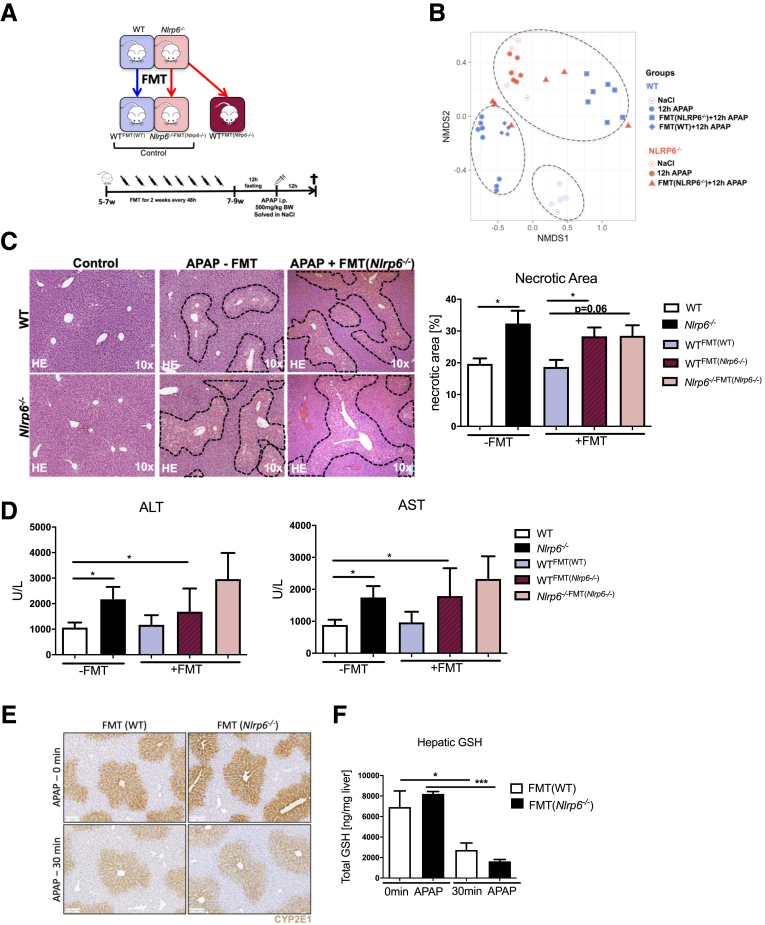
Results: Multivariate Cox regression analyses revealed a significantly increased risk (odds ratio, 2.3-3) for developing ALF in UK BioBank participants with PPI or ABx. Similarly, dysbiotic Nlrp6-/- mice displayed exacerbated APAP- and LPS-induced liver injury, which was linked to significantly reduced gut and liver tissue microbiota diversity and correlated with increased intestinal permeability at baseline. Fecal microbiota transfer (FMT) from Nlrp6-/- mice into wild-type (WT) mice augmented liver injury on APAP treatment in recipient WT mice, resembling the inflammatory phenotype of Nlrp6-/- mice. Specifically, FMT skewed monocyte polarization in WT mice toward a Ly6Chi inflammatory phenotype, suggesting a critical function of these cells as sensors of gut-derived signals orchestrating the inflammatory response.
Conclusions: Our data show an important yet unknown function of intestinal microbiota during ALF. Intestinal dysbiosis was transferrable to healthy WT mice via FMT and aggravated liver injury. Our study highlights intestinal microbiota as a targetable risk factor for ALF.
Keywords: Acute Liver Failure; Dysbiosis; Gut-Liver-Axis; Microbiota.
Copyright © 2021 The Authors. Published by Elsevier Inc. All rights reserved.
Figures







References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
