

Angiotensin-Converting Enzyme Inhibitor or Angiotensin Receptor Blocker Use Among Hypertensive US Adults With Albuminuria
- PMID: 33190561
- PMCID: PMC7725867
- DOI: 10.1161/HYPERTENSIONAHA.120.16281
Angiotensin-Converting Enzyme Inhibitor or Angiotensin Receptor Blocker Use Among Hypertensive US Adults With Albuminuria
Abstract
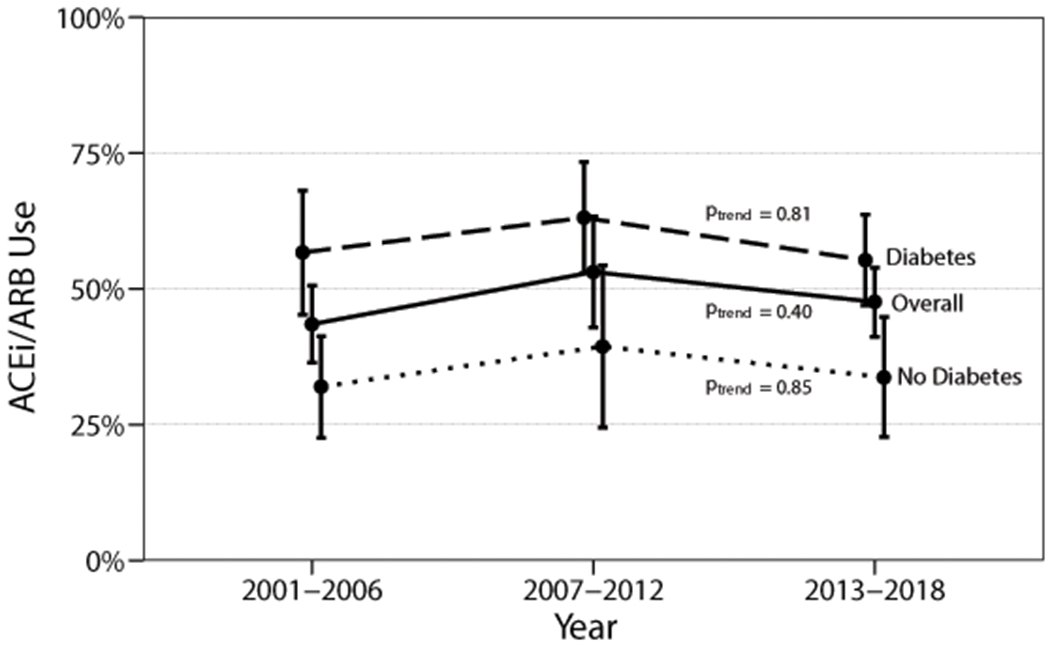
Since 2003, US hypertension guidelines have recommended ACE (angiotensin-converting enzyme) inhibitors or ARBs (angiotensin receptor blockers) as first-line antihypertensive therapy in the presence of albuminuria (urine albumin/creatinine ratio ≥300 mg/g). To examine national trends in guideline-concordant ACE inhibitor/ARB utilization, we studied adults participating in the National Health and Nutrition Examination Surveys 2001 to 2018 with hypertension (defined by self-report of high blood pressure, systolic blood pressure ≥140 mm Hg or diastolic ≥90 mm Hg, or use of antihypertensive medications). Among 20 538 included adults, the prevalence of albuminuria ≥300 mg/g was 2.8% in 2001 to 2006, 2.8% in 2007 to 2012, and 3.2% in 2013 to 2018. Among those with albuminuria ≥300 mg/g, no consistent trends were observed for the proportion receiving ACE inhibitor/ARB treatment from 2001 to 2018 among persons with diabetes, without diabetes, or overall. In 2013 to 2018, ACE inhibitor/ARB usage in the setting of albuminuria ≥300 mg/g was 55.3% (95% CI, 46.8%-63.6%) among adults with diabetes and 33.4% (95% CI, 23.1%-45.5%) among those without diabetes. Based on US population counts, these estimates represent 1.6 million adults with albuminuria ≥300 mg/g currently not receiving ACE inhibitor/ARB therapy, nearly half of whom do not have diabetes. ACE inhibitor/ARB underutilization represents a significant gap in preventive care delivery for adults with hypertension and albuminuria that has not substantially changed over time.
Keywords: albuminuria; angiotensin receptor antagonists; angiotensin-converting enzyme inhibitors; blood pressure; guideline adherence.
Conflict of interest statement
Figures
References
-
- Matsushita K, van der Velde M, Astor BC, Woodward M, Levey AS, de Jong PE, Coresh J, Gansevoort RT. Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality: a collaborative meta-analysis of general population cohorts. Lancet. 2010;375(9731):2073–2081. doi:10.1016/S0140-6736(10)60674-5 - DOI - PMC - PubMed
-
- Astor BC, Matsushita K, Gansevoort RT, van der Velde M, Woodward M, Levey AS, Jong PE de, Coresh J, Chronic Kidney Disease Prognosis Consortium, Astor BC, et al. Lower estimated glomerular filtration rate and higher albuminuria are associated with mortality and end-stage renal disease. A collaborative meta-analysis of kidney disease population cohorts. Kidney Int. 2011;79(12):1331–1340. doi:10.1038/ki.2010.550 - DOI - PMC - PubMed
-
- Matsushita K, Coresh J, Sang Y, Chalmers J, Fox C, Guallar E, Jafar T, Jassal SK, Landman GWD, Muntner P, et al. Estimated glomerular filtration rate and albuminuria for prediction of cardiovascular outcomes: a collaborative meta-analysis of individual participant data. Lancet Diabetes Endocrinol. 2015;3(7):514–525. doi:10.1016/S2213-8587(15)00040-6 - DOI - PMC - PubMed
-
- Hsu C, Chinchilli VM, Coca S, Devarajan P, Ghahramani N, Go AS, Hsu RK, Ikizler TA, Kaufman J, Liu KD, et al. Post–Acute Kidney Injury Proteinuria and Subsequent Kidney Disease Progression: The Assessment, Serial Evaluation, and Subsequent Sequelae in Acute Kidney Injury (ASSESS-AKI) Study. JAMA Intern Med. January 2020. doi:10.1001/jamainternmed.2019.6390 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
