

Risk stratification scores for patients with acute heart failure in the Emergency Department: A systematic review
- PMID: 33191763
- PMCID: PMC7886282
- DOI: 10.1177/2048872620930889
Risk stratification scores for patients with acute heart failure in the Emergency Department: A systematic review
Abstract
Aims: This study aimed to systematically identify and summarise all risk scores evaluated in the emergency department setting to stratify acute heart failure patients.
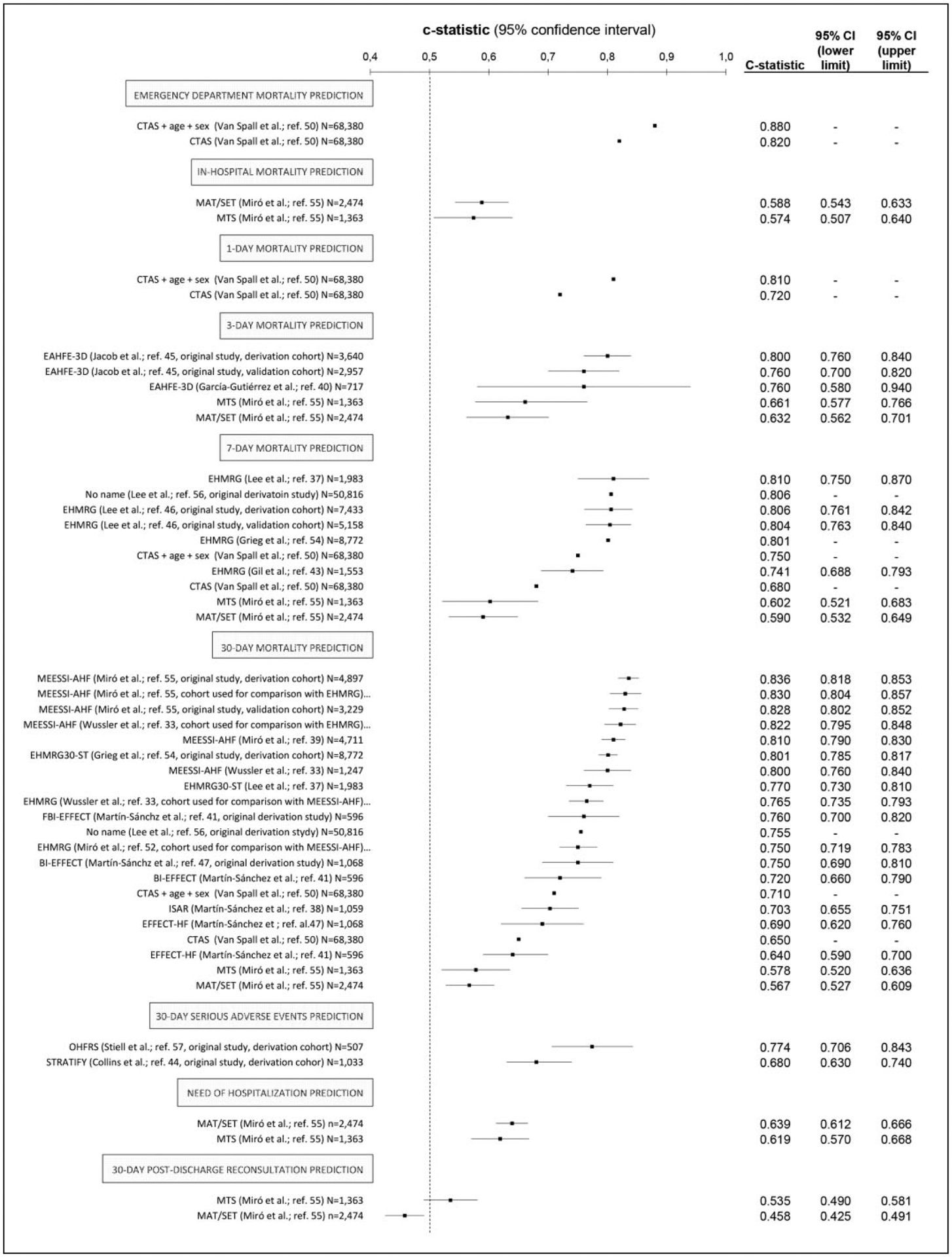
Methods and results: A systematic review of PubMed and Web of Science was conducted including all multicentre studies reporting the use of risk predictive models in emergency department acute heart failure patients. Exclusion criteria were: (a) non-original articles; (b) prognostic models without predictive purposes; and (c) risk models without consecutive patient inclusion or exclusively tested in patients admitted to a hospital ward. We identified 28 studies reporting findings on 19 scores: 13 were originally derived in the emergency department (eight exclusively using acute heart failure patients), and six in emergency department and hospitalised patients. The outcome most frequently predicted was 30-day mortality. The performance of the scores tended to be higher for outcomes occurring closer to the index acute heart failure event. The eight scores developed using acute heart failure patients only in the emergency department contained between 4-13 predictors (age, oxygen saturation and creatinine/urea included in six scores). Five scores (Emergency Heart Failure Mortality Risk Grade, Emergency Heart Failure Mortality Risk Grade 30 Day mortality ST depression, Epidemiology of Acute Heart Failure in Emergency department 3 Day, Acute Heart Failure Risk Score, and Multiple Estimation of risk based on Emergency department Spanish Score In patients with Acute Heart Failure) have been externally validated in the same country, and two (Emergency Heart Failure Mortality Risk Grade and Multiple Estimation of risk based on Emergency department Spanish Score In patients with Acute Heart Failure) further internationally validated. The c-statistic for Emergency Heart Failure Mortality Risk Grade to predict seven-day mortality was between 0.74-0.81 and for Multiple Estimation of risk based on Emergency department Spanish Score In patients with Acute Heart Failure to predict 30-day mortality was 0.80-0.84.
Conclusions: There are several scales for risk stratification of emergency department acute heart failure patients. Two of them are accurate, have been adequately validated and may be useful in clinical decision-making in the emergency department i.e. about whether to admit or discharge.
Keywords: Acute heart failure; emergency department; risk scores; systematic review.
Conflict of interest statement
Conflict of interest
The following authors provided statements of conflict of interests: Oscar Miró received grants from the Instituto de Salud Carlos III supported with funds from the Spanish Ministry of Health and FEDER (PI10/01918, PI11/01021, PI15/01019, PI15/00773, PI 18/00456), La Marató de TV3 (2015/2510) and from the Catalonian Government for Consolidated Groups of Investigation (GRC 2009/1385, 2014/0313, 2017/1424); Elke Platz received grants from the National Institutes of Health; Danielle M Gualandro has received research grants from FAPESP (Sao Paulo Research Foundation) and consulting honoraria from Roche, outside the submitted work; W Frank Peacock reports grants from Abbott, grants from Ortho Clinical Diagnostics, grants from Roche, grants and personal fees from Beckman Coulter, grants and personal fees from Siemens, grants and personal fees from Bayer, grants and personal fees from Quidel, outside the submitted work; John McMurray reports other from Bayer, non-financial support and other from Cardiorentis, non-financial support and other from Amgen, non-financial support and other from Oxford University/Bayer, non-financial support and other from Theracos, non-financial support and other from Abbvie, other from DalCor, other from Pfizer, other from Merck, non-financial support and other from Novartis, non-financial support and other from Glaxo Smith Kline (GSK), other from Bristol Myers Squibb (BMS), non-financial support and other from Vifor-Fresenius, non-financial support and other from Kidney Research UK (KRUK), non-financial support and other from Novartis, non-financial support and other from AstraZeneca, outside the submitted work; Louise Cullen reports grants and personal fees from Abbott Diagnostics, grants from Beckman Coulter, grants and personal fees from Siemens, outside the submitted work.; Francisco J Martın-Sanchez received speaker, advisory or consulting fees from Novartis, MSD, Bristol-Myers Squibb, Pfizer, The Medicine Company, Otsuka, Thermo Fisher, Cardiorentis, Sanofi and research grants from the Spanish Ministry of Health and FEDER, Mapfre, Novartis, Bayer, MSD, Abbot and Orion-Pharma; Martin R Cowie reports grants and personal fees from Abbott, grants and personal fees from Medtronic, grants and personal fees from Boston Scientific, personal fees from Servier, personal fees from Bayer, personal fees from Novartis, personal fees from AstraZeneca, personal fees from Fire1Foundry, personal fees from Neurotronik, outside the submitted work; Hector Bueno reports grants from Instituto de Salud Carlos III, personal fees from Bayer, personal fees from Novartis, grants, personal fees and non-financial support from AstraZeneca, grants and personal fees from BMS-Pfizer, personal fees from Ferrer, personal fees from MEDSCAPE-the Heart-org, personal fees from Janssen, outside the submitted work; Alexandre Mebazaa reports personal fees from Novartis, personal fees from Orion, personal fees from Roche, personal fees from Servier, grants and personal fees from Adrenomed, grants and personal fees from Abbott, personal fees from Sanofi, personal fees from Otsuka, personal fees from Philips, grants from 4TEEN4, outside the submitted work; Christian Mueller has received research support from the University Hospital Basel, the University of Basel, the Foundation for Cardiovascular Research Basel, the Swiss heart Foundation, the Swiss National Science Foundation, Abbott, Roche, Novartis and Singulex, as well as speaker honoraria from Novartis and Roche. Xavier Rossello, Josep Masip, Salvatore DiSomma, Mucio Tavares de Oliveira Jr, Alain S Maisel, Susanna Price and Christiaan Vrints have nothing to declare.
Figures



References
-
- Chioncel O, Mebazaa A, Harjola V-P, et al. Clinical phenotypes and outcome of patients hospitalized for acute heart failure: The ESC Heart Failure Long-Term Registry. Eur J Heart Fail 2017; 19: 1242–1254. - PubMed
-
- Llorens P, Javaloyes P, Martín-Sánchez FJ, et al. Time trends in characteristics, clinical course, and outcomes of 13,791 patients with acute heart failure. Clin Res Cardiol 2018; 107: 897–913. - PubMed
-
- Gayat E, Arrigo M, Littnerova S, et al. Heart failure oral therapies at discharge are associated with better outcome in acute heart failure: A propensity-score matched study. Eur J Heart Fail 2018; 20: 345–354. - PubMed
-
- Jencks SF, Williams MV and Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med 2009; 360: 1418–1428. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
