

Associated both-column acetabular fracture: An overview of operative steps and surgical technique
- PMID: 33192006
- PMCID: PMC7656469
- DOI: 10.1016/j.jcot.2020.08.027
Associated both-column acetabular fracture: An overview of operative steps and surgical technique
Abstract
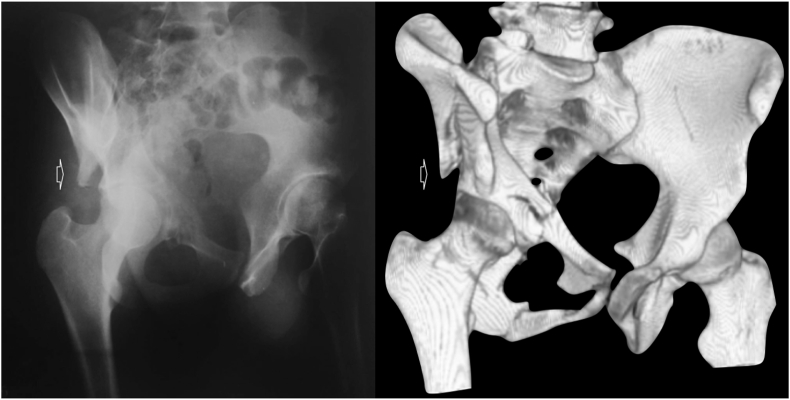
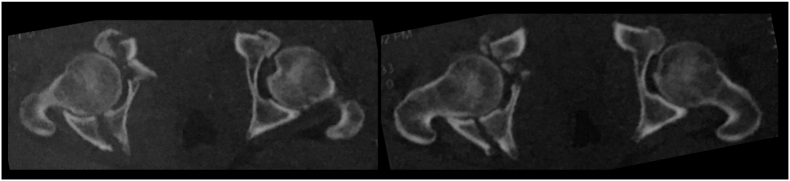
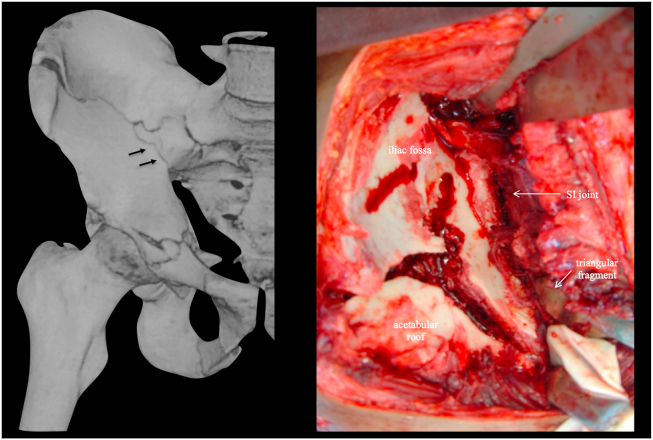
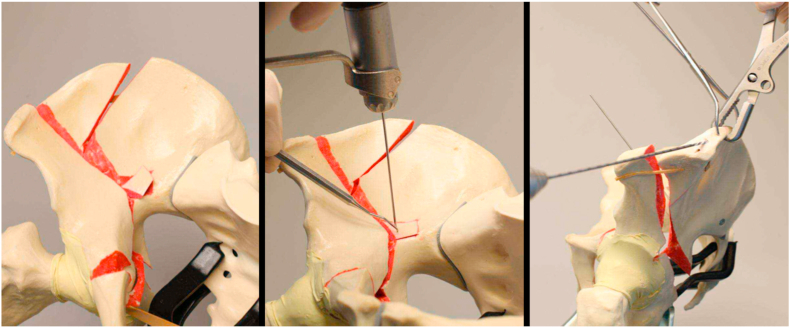
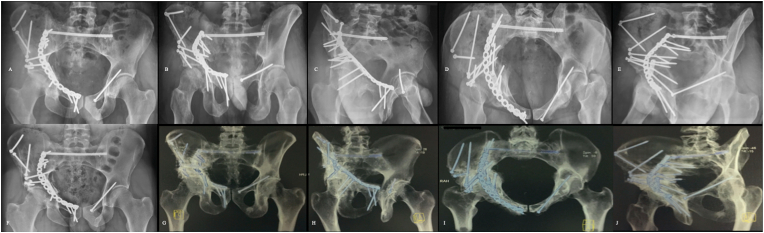
The management of both-column fractures of the acetabulum is challenging for the orthopaedic surgeon. Operative treatment is usually recommended in this particular fracture pattern, as residual joint surface displacement has been shown to increase local contact stress, drastically leading to rapid cartilage destruction. In this review, we present an overview of operative steps and surgical technique for both-column acetabular fracture reconstruction. Therefore, we demonstrate how correct understanding of fracture morphology and displacement, preoperative preparation, including choice of approach and patient positioning, reduction strategies, and programmed sequential fixation, starting from superior fracture lines on the anterior acetabular column and ending on the posterior components of this fracture type, may provide satisfactory outcomes in this difficult acetabular fracture pattern.
Keywords: Acetabular fracture; Approach to the acetabulum; Both-column acetabular fracture; Hip fracture.
Crown Copyright © 2020 All rights reserved.
Conflict of interest statement
None.
Figures


References
-
- Giannoudis P.V., Grotz M.R.W., Papakostidis C., Dinopoulos H. Operative treatment of displaced fractures of the acetabulum. A meta-analysis. J Bone Joint Surg Br. 2005;87(1):2–9. - PubMed
-
- Letournel E. Acetabulum fractures: classification and management. Clin Orthop Relat Res. 1980;(151):81–106. - PubMed
-
- Gänsslen A., Frink M., Hildebrand F., Krettek C. Both column fractures of the acetabulum: epidemiology, operative management and long-term-results. Acta Chir Orthop Traumatol Cech. 2012;79(2):107–113. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
