

Solutions for failed osteosynthesis of the acetabulum
- PMID: 33192007
- PMCID: PMC7656531
- DOI: 10.1016/j.jcot.2020.09.024
Solutions for failed osteosynthesis of the acetabulum
Erratum in
-
Erratum regarding previously published articles.J Clin Orthop Trauma. 2021 Oct;21:101559. doi: 10.1016/j.jcot.2021.101559. Epub 2021 Aug 5. J Clin Orthop Trauma. 2021. PMID: 34381301 Free PMC article.
Abstract
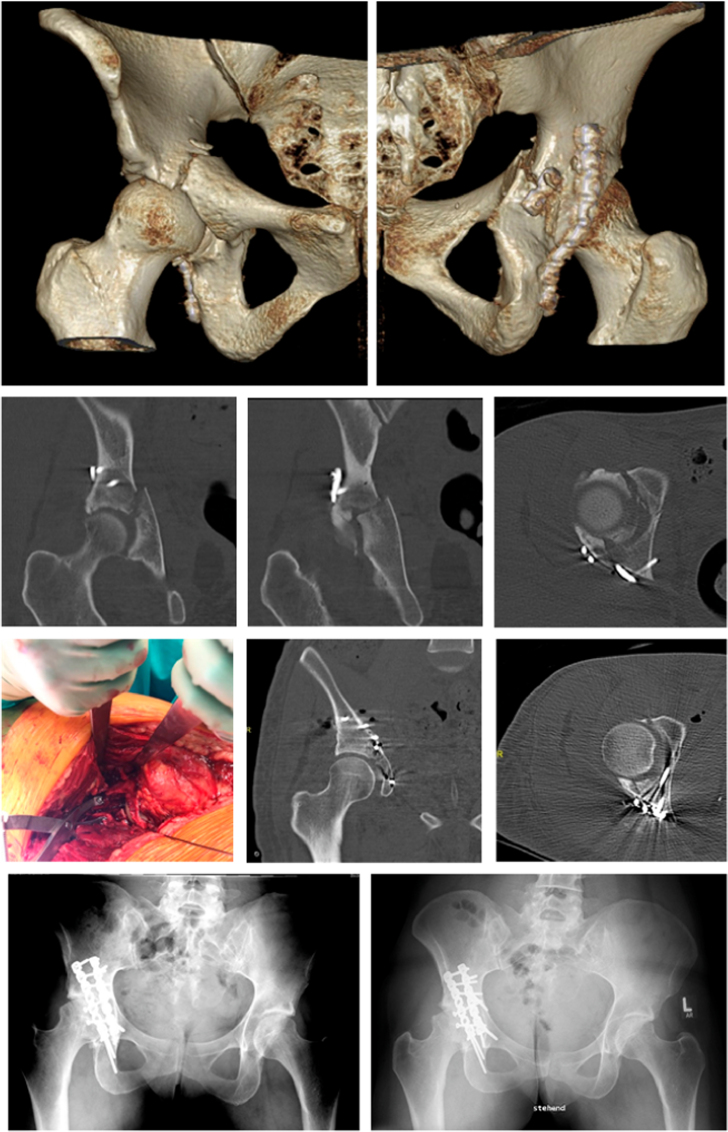
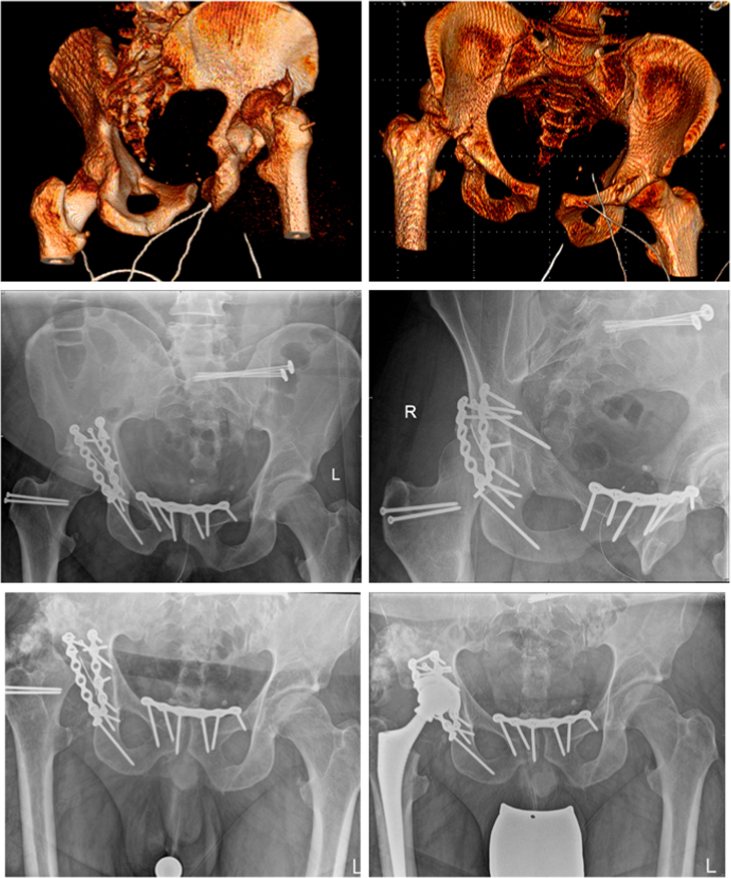
Osteosynthesis of the acetabulum is complex and requires very careful planning and preoperative preparation. The goal is to achieve anatomical reduction without steps or gaps in the articular surface. If it has not been possible to achieve an optimal reconstruction, one has to consider whether it makes sense to carry out reosteosynthesis or revise the fixation. The risk of infection, heterotopic ossification, avascular necrosis of the femur and cartilage damage is much higher than with the primary procedure. Often, especially in older patients, it may make more sense to achieve fracture union and to implant a total hip prosthesis in due course. In younger patients, every attempt should be made to achieve optimum anatomical reduction and this may mean consideration of reosteosynthesis after careful planning and counselling of the patient. If reosteosynthesis is considered adequate imaging including a postoperative CT is essential as part of the planning. This article looks at the possible solutions for failed osteosynthesis of the acetabulum.
Keywords: Acetabulum; Arthrosis; Hip prosthesis; Incongruency; Plate osteosynthesis; Reosteosynthesis.
© 2020.
Figures

References
-
- Gras F., Marintschev I., Grossterlinden L. The anterior intrapelvic approach for acetabular fractures using approach-specific instruments and an anatomical-preshaped 3-dimensional suprapectineal plate. J Orthop Trauma. 2017;31:e210–e216. - PubMed
-
- Letournel E. Acetabulum fractures: classification and management. Clin Orthop Relat Res. 1980:81–106. - PubMed
-
- O’Toole R.V., Hui E., Chandra A., Nascone J.W. How often does open reduction and internal fixation of geriatric acetabular fractures lead to hip arthroplasty? J Orthop Trauma. 2014;28:148–153. - PubMed
-
- Pennal G.F., Davidson J., Garside H., Plewes J. Results of treatment of acetabular fractures. Clin Orthop Relat Res. 1980:115–123. - PubMed
LinkOut - more resources
Full Text Sources
