

Anatomical quadrilateral plate for acetabulum fractures involving quadrilateral surface: A review
- PMID: 33192011
- PMCID: PMC7656483
- DOI: 10.1016/j.jcot.2020.10.013
Anatomical quadrilateral plate for acetabulum fractures involving quadrilateral surface: A review
Abstract
Introduction: The management of acetabulum fractures in osteoporotic elderly, as well as comminuted fractures in younger patients is likely to be difficult. These fractures need specific fixation techniques especially when the quadrilateral plate is involved. Standard implants may not be able to adequately support the fixation, so newer pre-shaped fixation plates have been proposed with some of these already in use. The concept of anatomic plates has come up for many fracture locations for providing a better buttress effect to the comminuted fragments. There has been a need to look for an anatomic buttress plates being developed for acetabulum fractures involving the quadrilateral surface.
Materials and methods: The literature has been reviewed to find the various newer designs that have been used for buttressing the quadrilateral surface in comminuted acetabular fractures. An attempt has been made to study their design characteristics and clinical outcomes. The review also includes the analysis of Anatomic Quadrilateral plate (AQP) used in fixation of acetabulum fracture involving quadrilateral surface in a series of 33 patients.
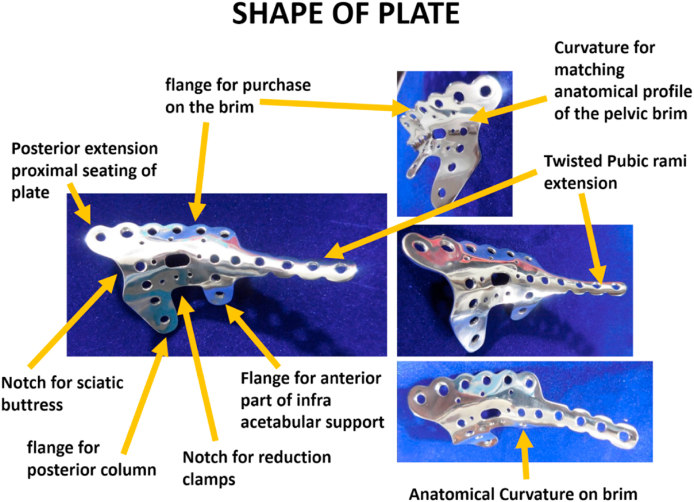
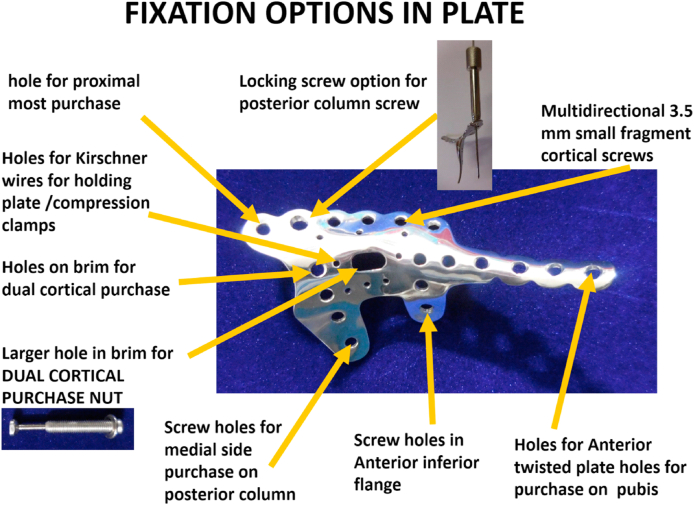
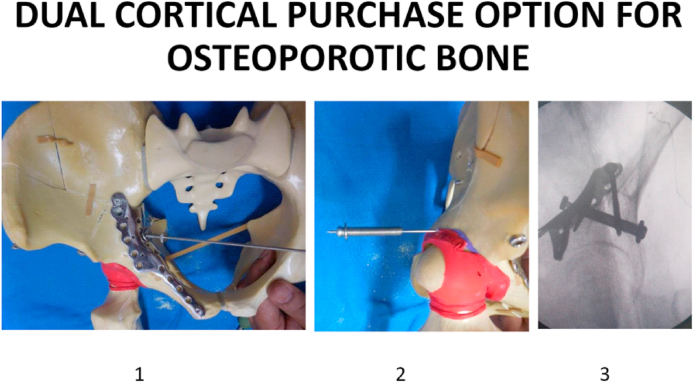
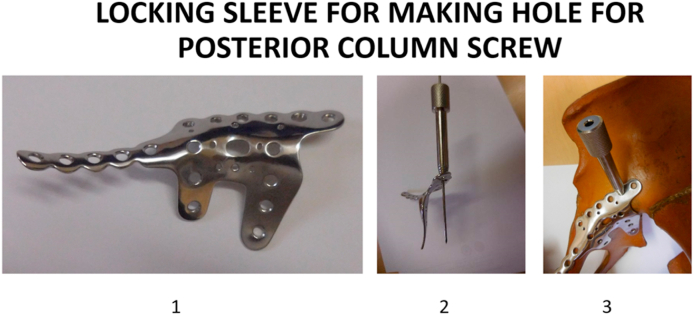
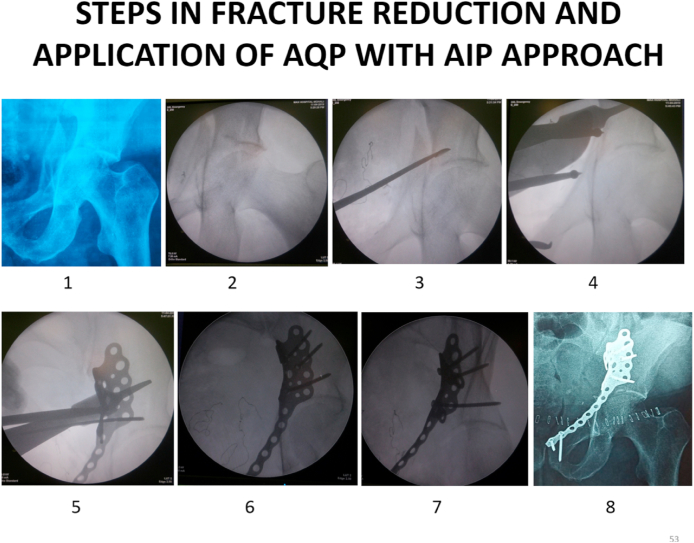
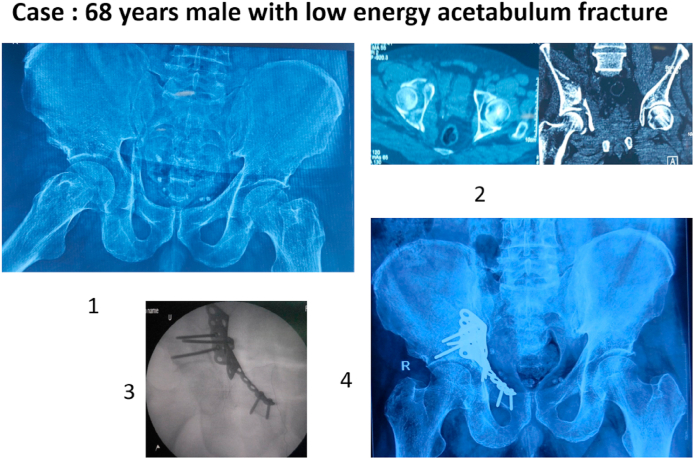
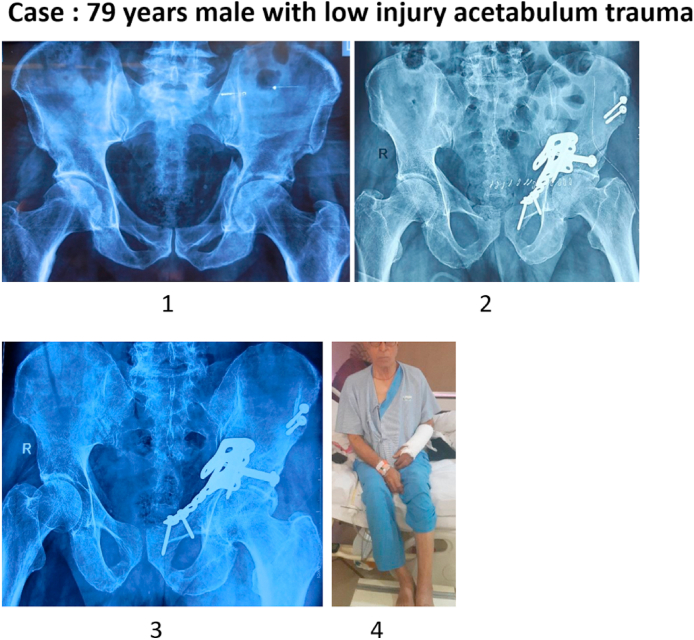
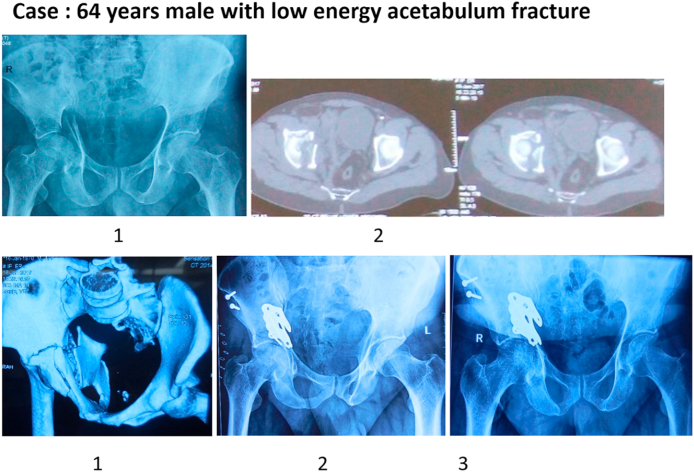
Results: There has been few anatomical plates developed for the stabilization of acetabular quadrilateral surface fractures. Some of these plates have been successfully used in management of acetabular fractures primarily in young patients. Issues however remain in their application and outcomes in osteoporotic fractures of the acetabulum, as these plates support the pelvic brim fragments either from superior or medial surface. The newer development i.e. 'Anatomical Quadrilateral Plate' is optimized to counter the displacement forces due to its positioning on the pelvic brim rather than its superior or medial surface. Other special features include the possibility of longer screws across bone due to oblique position of holes, the typical location of a locking hole on the plate beam which permits dual cortical compression fixation either by using a bigger screw or a specially designed screw in screw construct across the supra-acetabular corridor. The option of using hybrid fixation of both locking and unlocked screws in AQP allows proper stress distribution on the underlying bone, aiding both primary as well as secondary stability. The minimum of one year post surgery outcome of patients having acetabular fixation using this Anatomic quadrilateral plate has been analyzed in 33 patients. Twenty three of these were aged more than 50 years and 28 out of total 33 were males. Associated injuries included Ipsilateral lower limb injury in 2 patients and distal radius fracture in 5 patients. The fracture pattern included 'Anterior column posterior hemi-transverse' in 10 patients,' Associated Both Column' injury in 9 and 'T type' acetabular fractures in 8 patients. Isolated 'Anterior column' was fractured in 6 patients. The surgical approach was 'Anterior Intra-pelvic' (AIP) in 23 patients and 'Modified Ileo-femoral' in other 10 patients. One patient had additional K L approach. Among the implants, the AQP plate was used without its pubic arm in 6 patients. The post-operative x rays showed anatomical reduction in 28 patients, while other 5 had gaps and/or steps up to 2 mm size. In subsequent car, one of these patients needed hip arthroplasty for problem arising due to collapse in fixation within six months. EQ 5D 5L telephonic score was used to know the outcome at minimum of one year follow up in 33 patients. As per this score, only 3 patients had an issue with mobility, with only one having problem in self-care activity. Six patients complained of minor limitations in carrying out their usual activities and only one patient had anxiety affecting him. In their self-assessment of overall health status, 22 patients marked it 100, 7 made it 90, 3 as 80 and 1 had marked it as 70 in a score range of 0-100. Considering the predominant elderly profile in this series of patients, the acetabular reconstruction using 'Anatomic quadrilateral plate' has shown encouraging results.
Conclusion: For stabilization of acetabular fractures involving quadrilateral surface area and pelvic brim, various new implants have been used. The Anatomic quadrilateral plate due to its anatomical shape, the various options in fracture fixation is best optimized for management of comminuted acetabulum fractures especially in poor quality bones. It has been successful in achieving good outcome in elderly group of patients having these complex injuries.
Keywords: Acetabulum fracture; Anatomical plate; Anterior column fractures; Comminution; Dual cortical fixation; Osteoporosis; Quadrilateral plate fractures.
© 2020 Delhi Orthopedic Association. All rights reserved.
Conflict of interest statement
The authors have none to declare.
Figures
References
-
- Henry P.D.G., Kreder H.J., Jenkinson R.J. The osteoporotic acetabular fracture orthop. Clin N Am. 2013;44:201–215. - PubMed
-
- Lansinger O., Romanus B., Goldie I.F. Fracture mechanism in central acetabular fractures. Arch Orthop Trauma Surg. 1979;94:209–212. - PubMed
-
- Ferguson T.A., Patel R., Bhandari M., Matta J.M. Fractures of the acetabulum in patients aged 60 years and older. J Bone Joint Surg. 2020;92B:250–257. - PubMed
-
- Matta J.M. Fractures of the acetabulum: accuracy of reduction and clinical results in patients managed operatively within three weeks after injury. J Bone Joint Surg. 1996;78A:1632–1645. - PubMed
-
- Miller A.N., Prasarn M.L., Lorich D.G. The radiological evaluation of acetabular fractures in the elderly. J Bone Joint Surg. 2010;92-B:560–564. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
