

The Distribution of Alpha-1 Antitrypsin Genotypes Between Patients with COPD/Emphysema, Asthma and Bronchiectasis
- PMID: 33192056
- PMCID: PMC7654539
- DOI: 10.2147/COPD.S271810
The Distribution of Alpha-1 Antitrypsin Genotypes Between Patients with COPD/Emphysema, Asthma and Bronchiectasis
Abstract
Purpose: Alpha-1-antitrypsin deficiency (AATD) is a rare hereditary condition characterized by low circulating levels of alpha-1antitrypsin (AAT). While the association between AATD and COPD/emphysema is undisputed, the association between AATD and asthma or bronchiectasis is still a matter of debate.
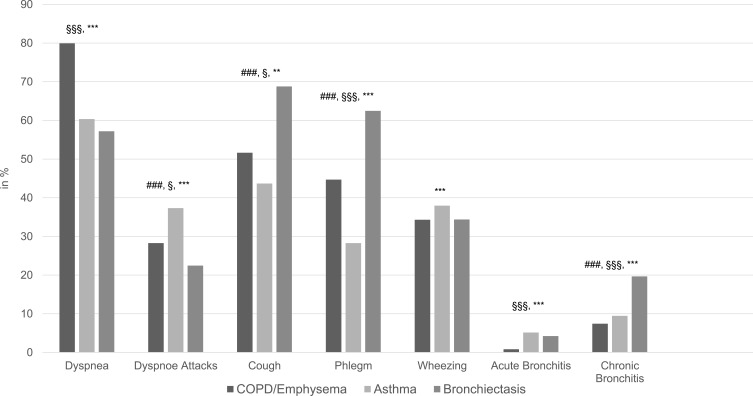
Aims and objectives: Our study aimed to investigate the distribution of AAT genotypes between patients with COPD/emphysema, asthma and bronchiectasis. To back up the diagnostic labels, we described symptoms associated with the diagnosis.
Methods: Between September 2003 and March 2020, 29,465 testing kits (AlphaKit®) were analyzed in the AAT laboratory, University of Marburg, Germany. The diagnosis of AATD has been made based on the measurements of AAT serum levels, followed by genotyping, phenotyping or whole gene sequencing depending on the availability and/or the need for more detailed interpretation of the results. The respiratory symptoms were recorded as well.
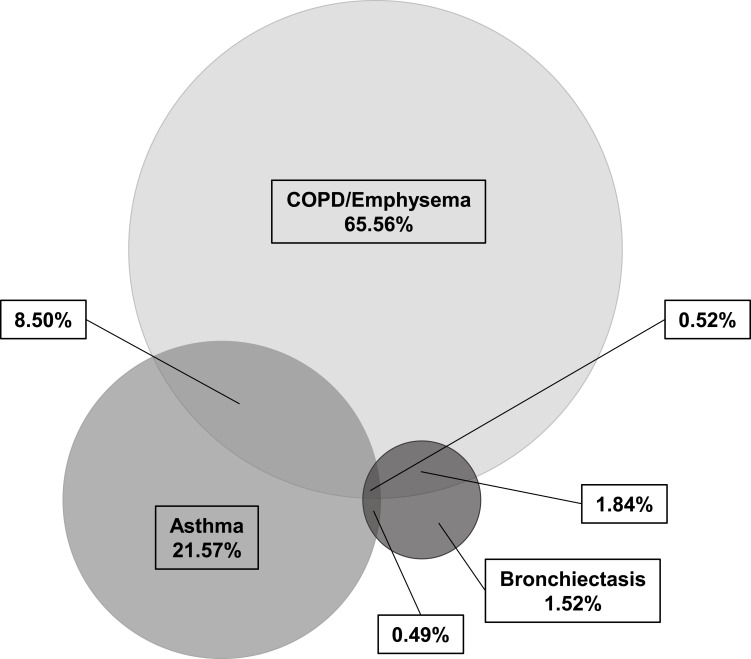
Results: Regarding the distribution of the wild type allele M and the most frequent mutations S (E264V) and Z (E342K), no significant differences could be found between COPD/emphysema [Pi*MM (58.24%); Pi*SZ (2.49%); Pi*ZZ (9.12%)] and bronchiectasis [Pi*MM (59.30%) Pi*SZ (2.81%); Pi*ZZ (7.02%)]. When COPD/emphysema and bronchiectasis were recorded in the same patient, the rate of Pi* ZZ (14.78%) mutations was even higher. Asthma patients exhibited significantly less deficient genotypes [Pi*MM (54.81%); Pi*SZ (2%); Pi*ZZ (2.77%)] than two other groups. Associated respiratory symptoms confirmed the diagnosis.
Conclusion: COPD/emphysema and bronchiectasis, but not asthma patients, exhibit higher frequency of AATD genotypes. Our data suggest that AATD testing should be offered to patients with COPD/emphysema and bronchiectasis.
Keywords: SERPINA1; alpha-1-antitrypsin deficiency; asthma; bronchiectasis; diagnosis.
© 2020 Veith et al.
Conflict of interest statement
Martina Veith reports grants from Grifols. Prof. Dr. Robert Bals reports grants from BMBF, during the conduct of the study; grants from Schwiete Stiftung, Novartis, and Mukoviszidose e.V. and personal fees from AstraZeneca and CSL Behring, outside the submitted work. Prof. Dr. Claus Franz Vogelmeier reports grants, personal fees from AstraZeneca, Boehringer Ingelheim, Grifols, GlaxoSmithKline, and Novartis; personal fees from CSL Behring, Chiesi, Menarini, Nuvaira, MedUpdate, outside the submitted work. Dr Timm Greulich reports grants from Grifols, during the conduct of the study; personal fees from AstraZeneca, serves as a lecturer and part of the advisory board for Berlin Chemie, Boehringer Ingelheim, Chiesi, CSL Behring, Grifols, GSK, Novartis, received grants from German Centre for Lung Research, outside the submitted work. The authors report no other conflicts of interest in this work.
Figures



Similar articles
-
An Alpha-1 Antitrypsin Deficiency Screening Study in Patients with Chronic Obstructive Pulmonary Disease, Bronchiectasis, or Asthma in Turkey.Int J Chron Obstruct Pulmon Dis. 2023 Nov 28;18:2785-2794. doi: 10.2147/COPD.S425835. eCollection 2023. Int J Chron Obstruct Pulmon Dis. 2023. PMID: 38046982 Free PMC article.
-
Frequency of alleles and genotypes associated with alpha-1 antitrypsin deficiency in clinical and general populations: Revelations about underdiagnosis.Pulmonology. 2023 May-Jun;29(3):214-220. doi: 10.1016/j.pulmoe.2022.01.017. Epub 2022 Mar 26. Pulmonology. 2023. PMID: 35346640
-
Results from a large targeted screening program for alpha-1-antitrypsin deficiency: 2003 - 2015.Orphanet J Rare Dis. 2016 Jun 10;11(1):75. doi: 10.1186/s13023-016-0453-8. Orphanet J Rare Dis. 2016. PMID: 27282198 Free PMC article.
-
Alpha-1 Antitrypsin Deficiency.2006 Oct 27 [updated 2023 Jun 1]. In: Adam MP, Feldman J, Mirzaa GM, Pagon RA, Wallace SE, Amemiya A, editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993–2025. 2006 Oct 27 [updated 2023 Jun 1]. In: Adam MP, Feldman J, Mirzaa GM, Pagon RA, Wallace SE, Amemiya A, editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993–2025. PMID: 20301692 Free Books & Documents. Review.
-
Hereditary alpha-1-antitrypsin deficiency and its clinical consequences.Orphanet J Rare Dis. 2008 Jun 19;3:16. doi: 10.1186/1750-1172-3-16. Orphanet J Rare Dis. 2008. PMID: 18565211 Free PMC article. Review.
Cited by
-
Alpha-1 Antitrypsin Screening in a Selected Cohort of Patients Affected by Chronic Pulmonary Diseases in Naples, Italy.J Clin Med. 2021 Apr 7;10(8):1546. doi: 10.3390/jcm10081546. J Clin Med. 2021. PMID: 33916947 Free PMC article.
-
Bronchiectasis-COPD Overlap Syndrome: A Comprehensive Review of its Pathophysiology and Potential Cardiovascular Implications.Ther Adv Pulm Crit Care Med. 2024 Dec 9;19:29768675241300808. doi: 10.1177/29768675241300808. eCollection 2024 Jan-Dec. Ther Adv Pulm Crit Care Med. 2024. PMID: 39655338 Free PMC article. Review.
-
Feasibility of a genotyping system for the diagnosis of alpha1 antitrypsin deficiency: a multinational cross-sectional analysis.Respir Res. 2022 Jun 10;23(1):152. doi: 10.1186/s12931-022-02074-x. Respir Res. 2022. PMID: 35689213 Free PMC article.
-
Hidden Comorbidities in Asthma: A Perspective for a Personalized Approach.J Clin Med. 2023 Mar 15;12(6):2294. doi: 10.3390/jcm12062294. J Clin Med. 2023. PMID: 36983294 Free PMC article. Review.
-
Nine controversial questions about augmentation therapy for alpha-1 antitrypsin deficiency: a viewpoint.Eur Respir Rev. 2023 Dec 6;32(170):230170. doi: 10.1183/16000617.0170-2023. Print 2023 Dec 31. Eur Respir Rev. 2023. PMID: 38056890 Free PMC article.
References
-
- Janciauskiene SM, Bals R, Koczulla R, Vogelmeier C, Kohnlein T, Welte T. The discovery of alpha1-antitrypsin and its role in health and disease. Respir Med. 2011;105(8):1129–1139. - PubMed
-
- European RS, American Thoracic Society. American thoracic society/European respiratory society statement: standards for the diagnosis and management of individuals with alpha-1 antitrypsin deficiency. Am J Respir Crit Care Med. 2003;168(7):818–900. - PubMed
-
- Stoller JK, Brantly M. The challenge of detecting alpha-1 antitrypsin deficiency. Copd. 2013;10(Suppl 1):26–34. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
