

Beta-Adrenergic Receptor Stimulation Modulates the Cellular Proarrhythmic Effects of Chloroquine and Azithromycin
- PMID: 33192602
- PMCID: PMC7642988
- DOI: 10.3389/fphys.2020.587709
Beta-Adrenergic Receptor Stimulation Modulates the Cellular Proarrhythmic Effects of Chloroquine and Azithromycin
Abstract
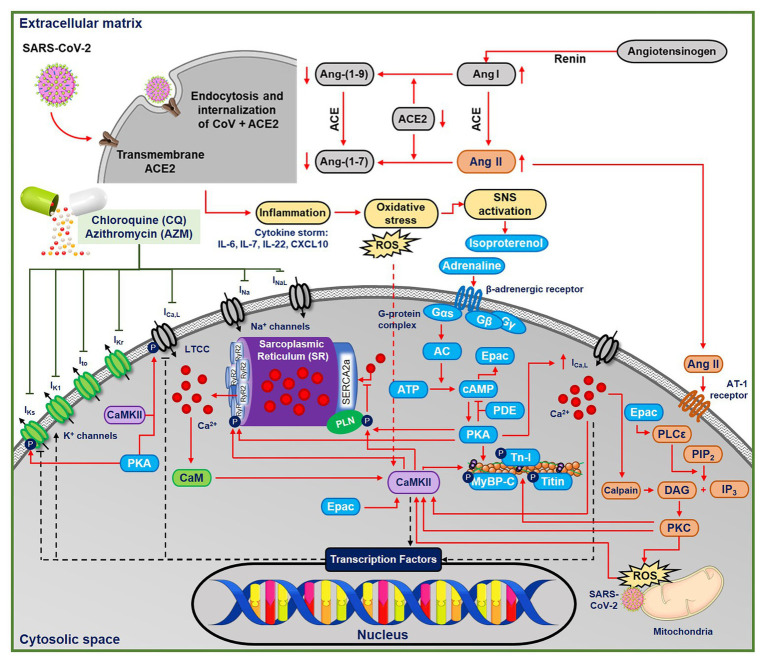
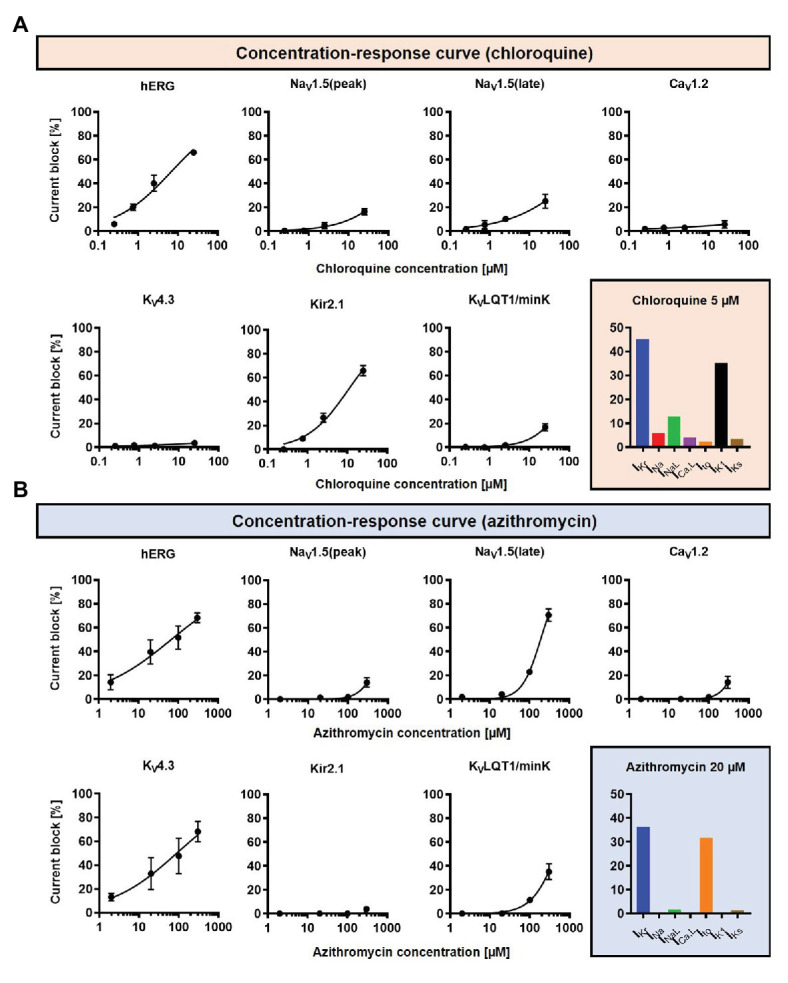
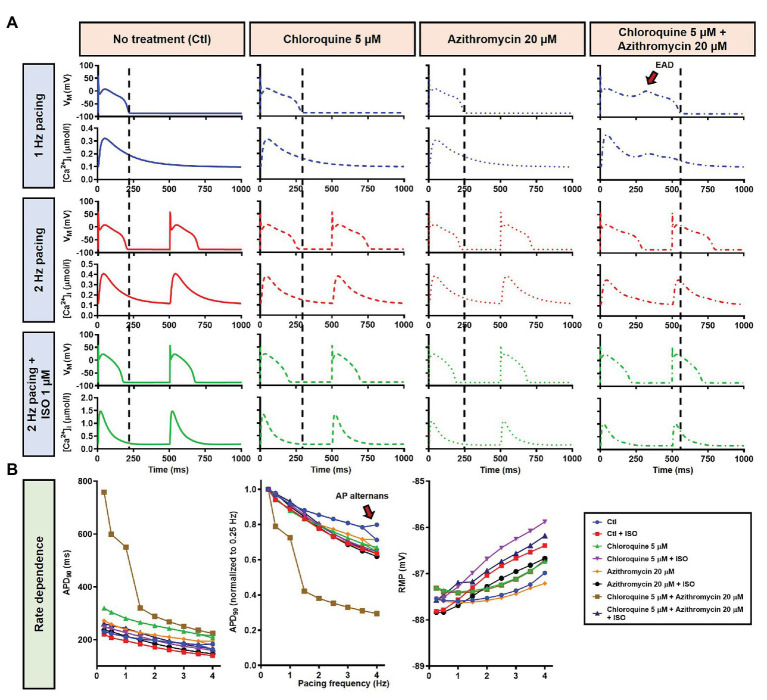
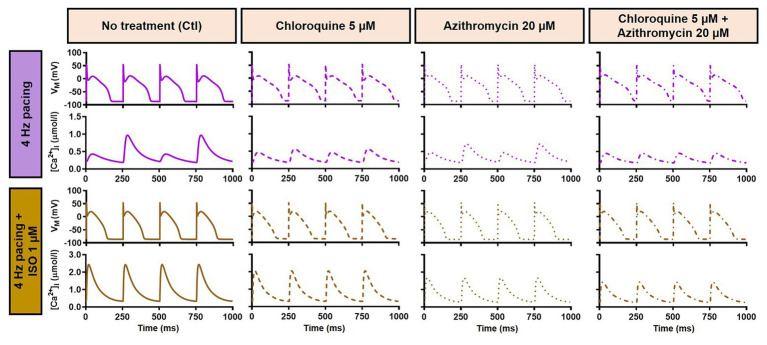
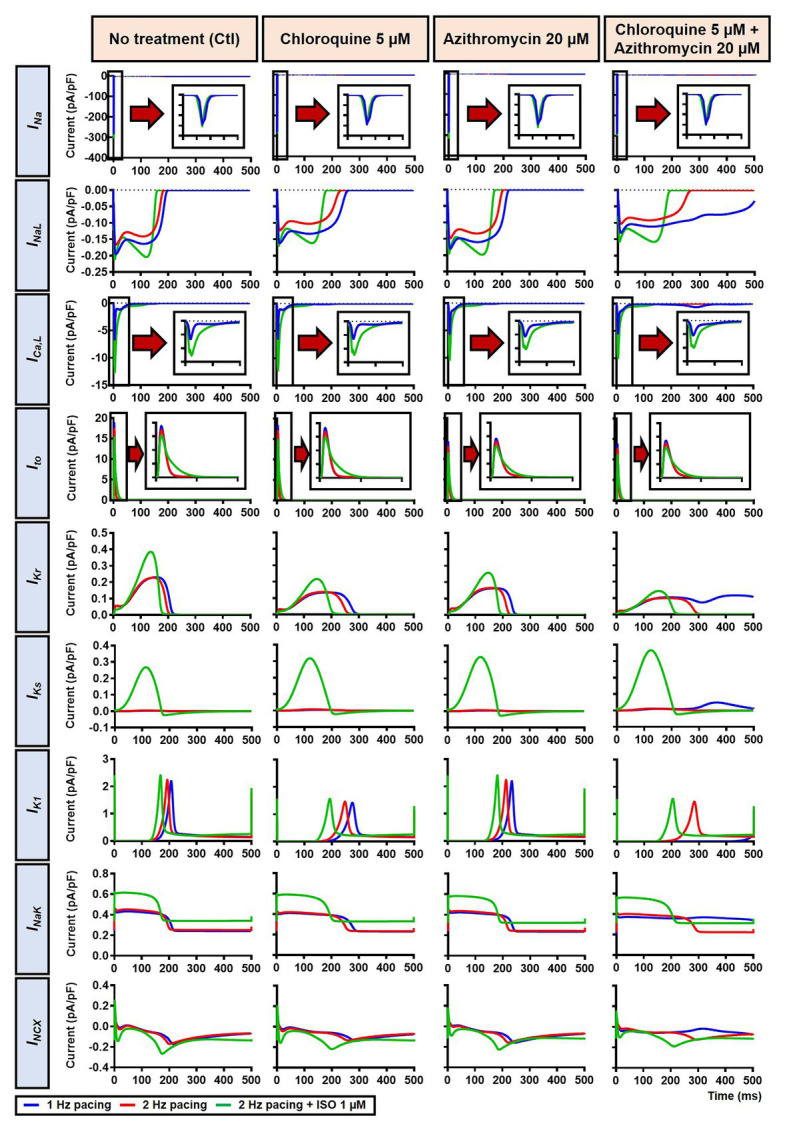
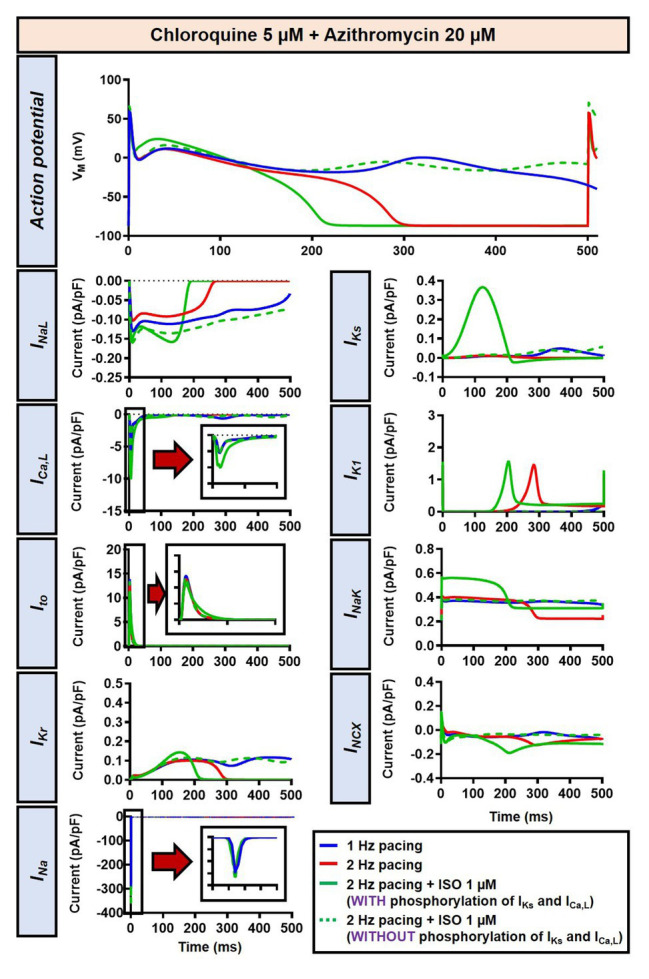
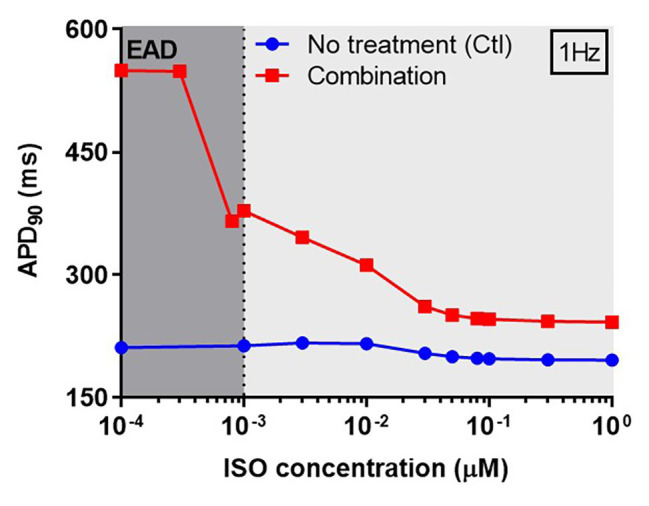
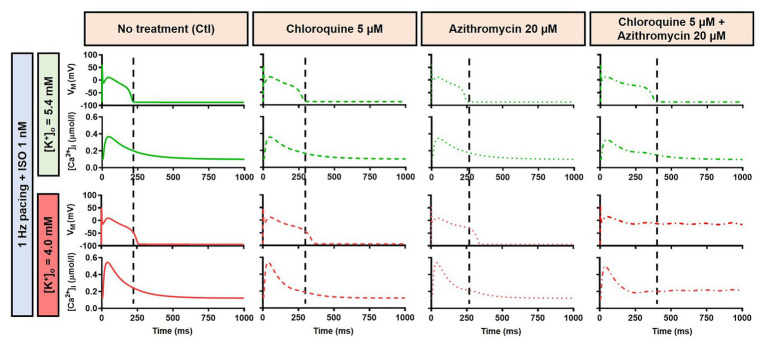
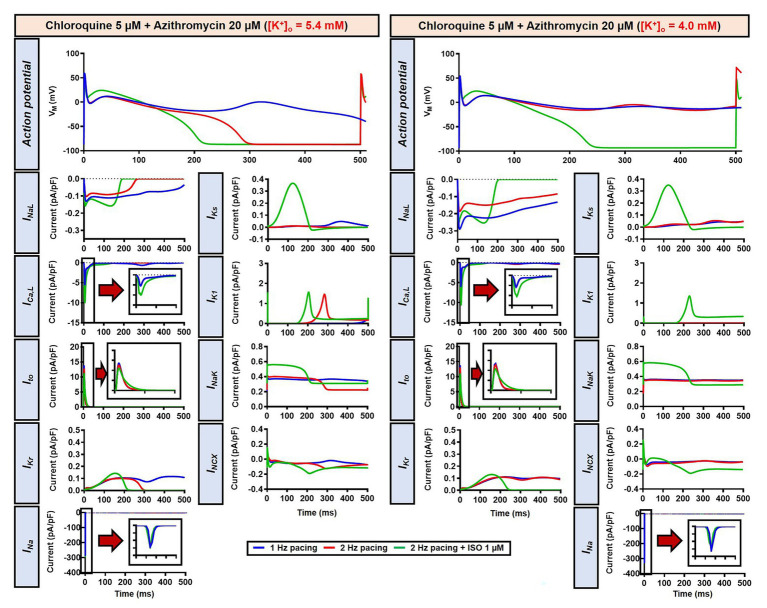
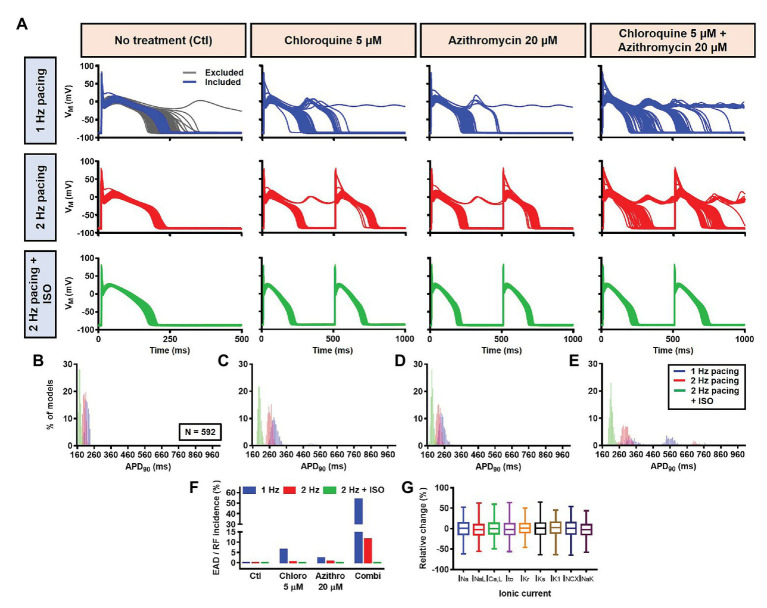
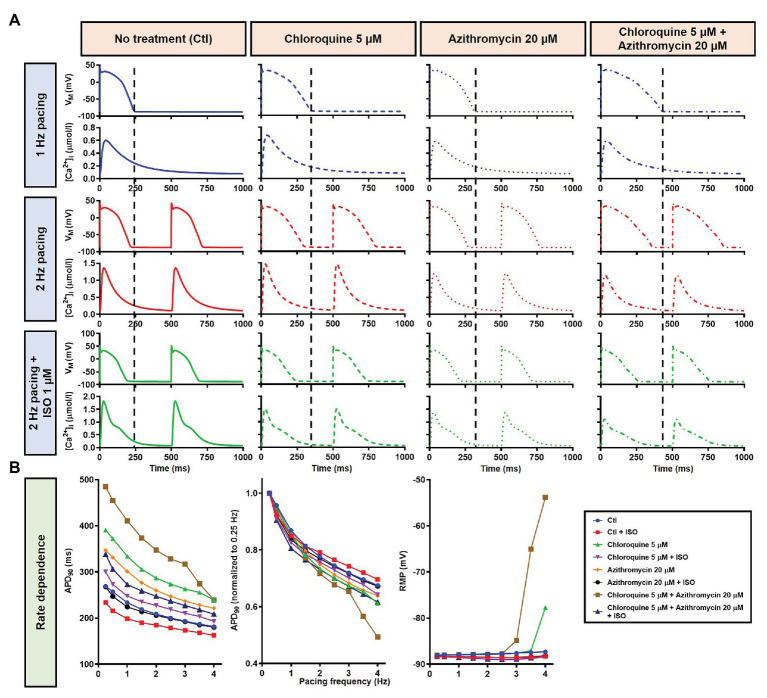
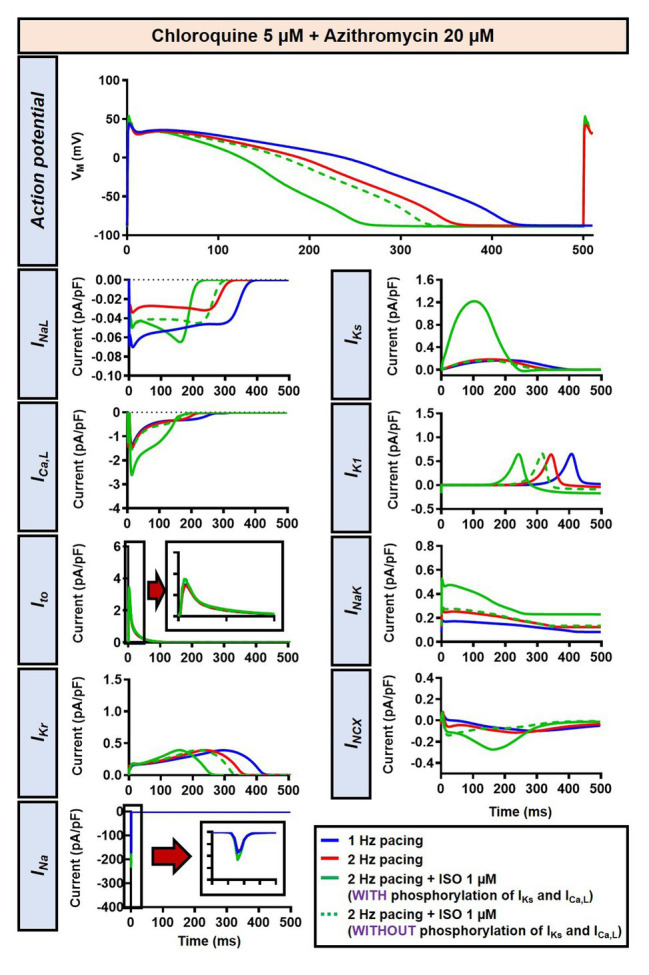
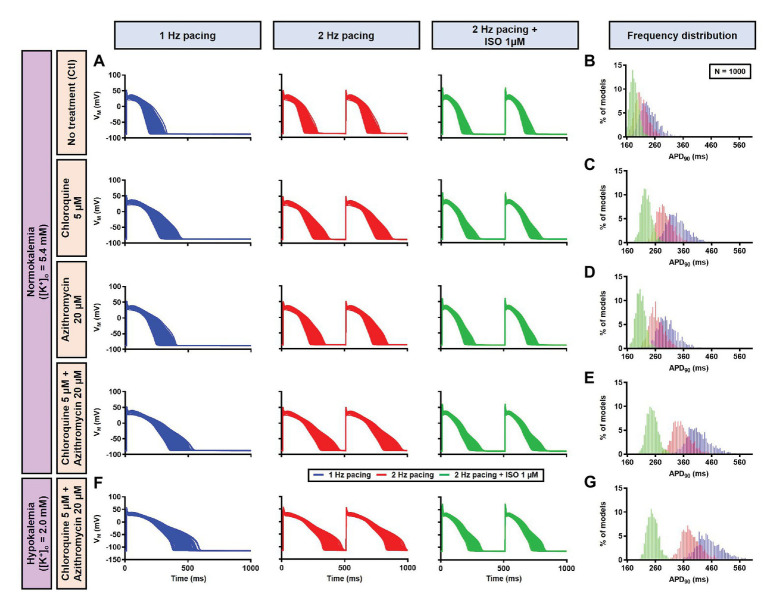
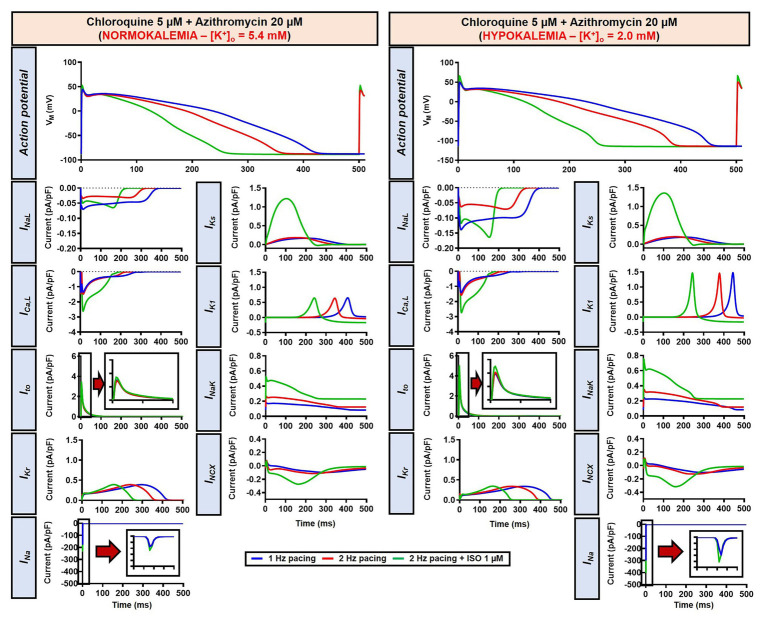
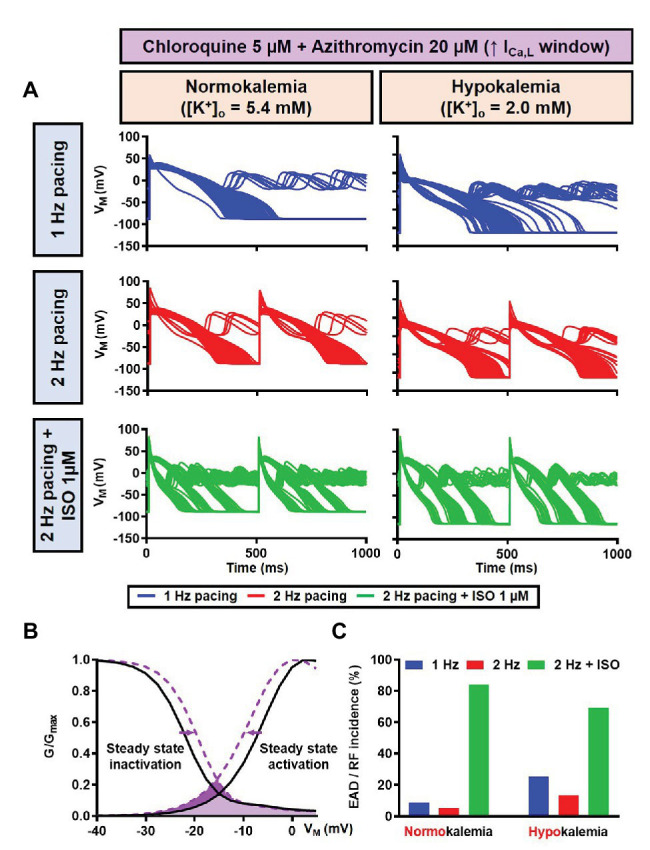
The antimalarial drug, chloroquine (CQ), and antimicrobial drug, azithromycin (AZM), have received significant attention during the COVID-19 pandemic. Both drugs can alter cardiac electrophysiology and have been associated with drug-induced arrhythmias. Meanwhile, sympathetic activation is commonly observed during systemic inflammation and oxidative stress (e.g., in SARS-CoV-2 infection) and may influence the electrophysiological effects of CQ and AZM. Here, we investigated the effect of beta-adrenergic stimulation on proarrhythmic properties of CQ and AZM using detailed in silico models of ventricular electrophysiology. Concentration-dependent alterations in ion-channel function were incorporated into the Heijman canine and O'Hara-Rudy human ventricular cardiomyocyte models. Single and combined drug effects on action-potential (AP) properties were analyzed using a population of 1,000 models accommodating inter-individual variability. Sympathetic stimulation was simulated by increasing pacing rate and experimentally validated isoproterenol (ISO)-induced changes in ion-channel function. In the canine ventricular model at 1 Hz pacing, therapeutic doses of CQ and AZM (5 and 20 μM, respectively) individually prolonged AP duration (APD) by 33 and 13%. Their combination produced synergistic APD prolongation (+161%) with incidence of proarrhythmic early afterdepolarizations in 53.5% of models. Increasing the pacing frequency to 2 Hz shortened APD and together with 1 μM ISO counteracted the drug-induced APD prolongation. No afterdepolarizations occurred following increased rate and simulated application of ISO. Similarly, CQ and AZM individually prolonged APD by 43 and 29% in the human ventricular cardiomyocyte model, while their combination prolonged APD by 76% without causing early afterdepolarizations. Consistently, 1 μM ISO at 2 Hz pacing counteracted the drug-induced APD prolongation. Increasing the ICa,L window current produced afterdepolarizations, which were exacerbated by ISO. In both models, reduced extracellular K+ reduced the repolarization reserve and increased drug effects. In conclusion, CQ- and AZM-induced proarrhythmia is promoted by conditions with reduced repolarization reserve. Sympathetic stimulation limits drug-induced APD prolongation, suggesting the potential importance of heart rate and autonomic status monitoring in particular conditions (e.g., COVID-19).
Keywords: COVID-19; arrhythmia; azithromycin; beta-adrenergic; chloroquine; computational modeling; electrophysiology-basic.
Copyright © 2020 Sutanto and Heijman.
Figures
References
-
- Bartos D. C., Giudicessi J. R., Tester D. J., Ackerman M. J., Ohno S., Horie M., et al. (2014). A KCNQ1 mutation contributes to the concealed type 1 long QT phenotype by limiting the Kv7.1 channel conformational changes associated with protein kinase A phosphorylation. Heart Rhythm 11, 459–468. 10.1016/j.hrthm.2013.11.021, PMID: - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous