

Three-Dimensional Printing Assisted Laparoscopic Partial Nephrectomy vs. Conventional Nephrectomy in Patients With Complex Renal Tumor: A Systematic Review and Meta-Analysis
- PMID: 33194610
- PMCID: PMC7643019
- DOI: 10.3389/fonc.2020.551985
Three-Dimensional Printing Assisted Laparoscopic Partial Nephrectomy vs. Conventional Nephrectomy in Patients With Complex Renal Tumor: A Systematic Review and Meta-Analysis
Abstract
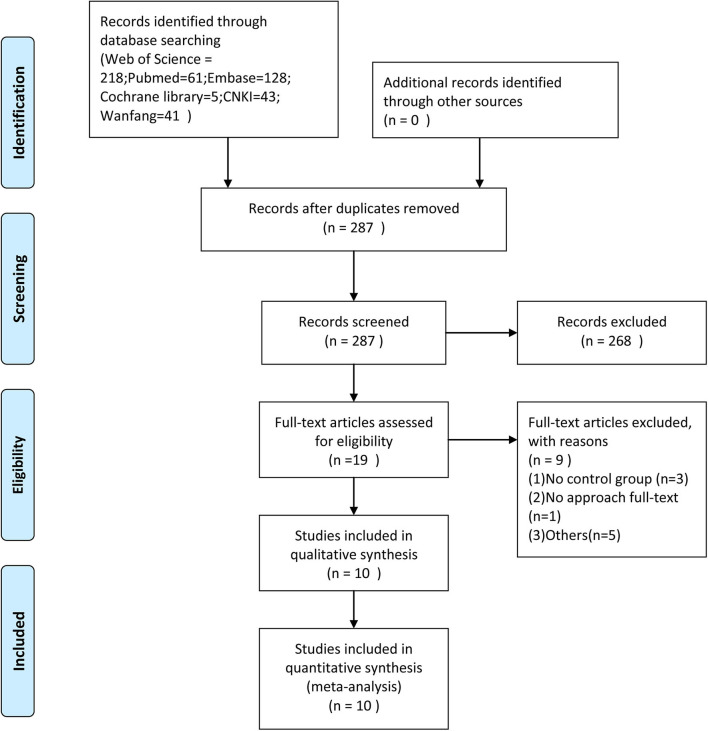
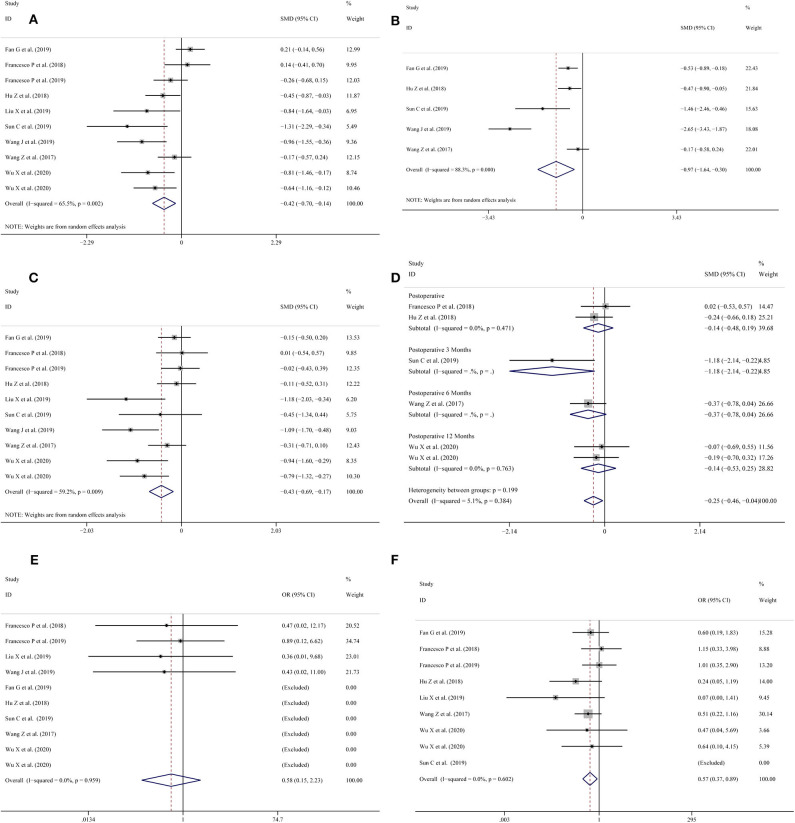
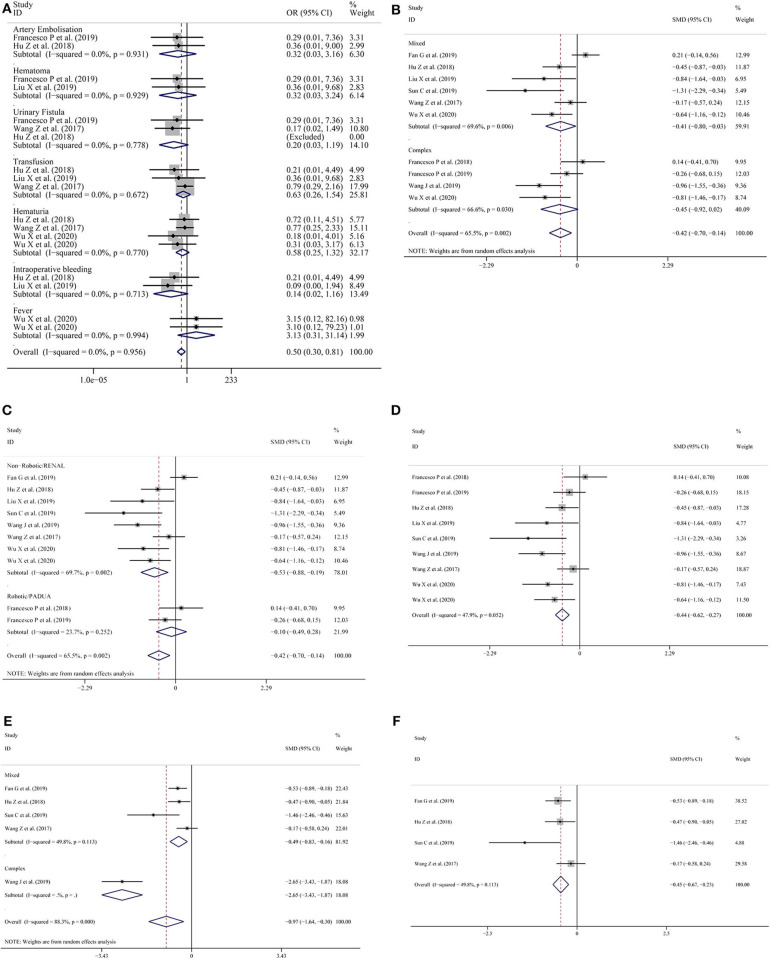
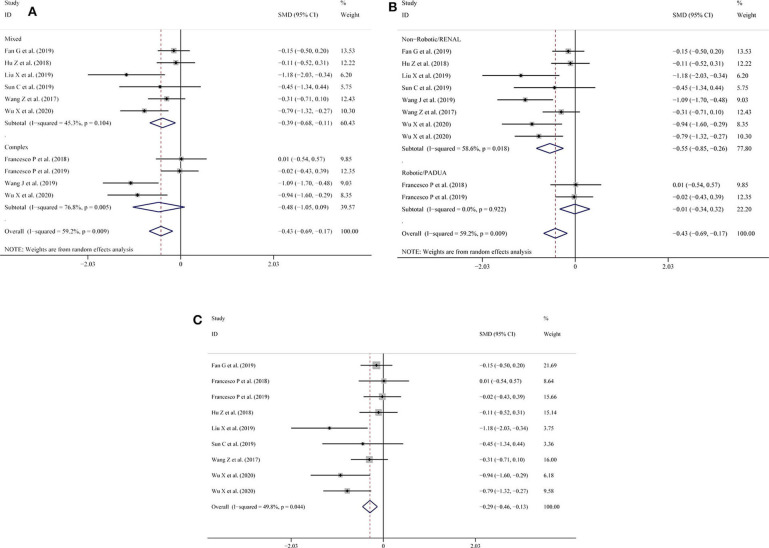
Objective: The purpose of this meta-analysis was to systematically assess the influence of three-dimensional (3D) printing technology in laparoscopic partial nephrectomy (LPN) of complex renal tumors. Methods: A systematic literature review was performed in June 2020 using the Web of Science, PubMed, Embase, the Cochrane library, the China National Knowledge Infrastructure (CNKI), and the Wanfang Databases to identify relevant studies. The data relative to operation time, warm ischemic time, intraoperative blood loss, positive surgical margin, reduction in estimated glomerular filtration rate (eGFR), and complications (including artery embolization, hematoma, urinary fistula, transfusion, hematuria, intraoperative bleeding, and fever) were extracted. Two reviewers independently assessed the quality of all included studies, and the eligible studies were included and analyzed using the Stata 12.1 software. A subgroup analysis was performed stratifying patients according to the complexity of the tumor and surgery type or to the nephrometry score. Results: One randomized controlled trial (RCT), two prospective controlled studies (PCS), and seven retrospective comparative studies (RCS) were analyzed, involving a total of 647 patients. Our meta-analysis showed that there were significant differences in operation time, warm ischemic time, intraoperative blood loss, reduction in eGFR, and complications between the LPN with 3D-preoperative assessment (LPN-3DPA) vs. LPN with conventional 2D preoperative assessment (LPN-C2DPA) groups. Positive surgical margin did not differ significantly. Conclusion: The LPN-3DPA group showed shorter operation time and warm ischemic time, as well as less intraoperative blood loss, reduction in eGFR, fewer complications for patients with complex renal tumor. Therefore, LPN assisted by three-dimensional printing technology should be a preferable treatment of complex renal tumor when compared with conventional LPN. However, further large-scale RCTs are needed in the future to confirm these findings.
Keywords: complex renal tumor; eGFR; laparoscopic partial nephrectomy; meta-analysis; three-dimensional printing.
Copyright © 2020 Jiang, Zeng, Zhu, Chen and Chen.
Figures
Similar articles
-
Comparison of Renal Artery vs Renal Artery-Vein Clamping During Partial Nephrectomy: A System Review and Meta-Analysis.J Endourol. 2020 Apr;34(4):523-530. doi: 10.1089/end.2019.0580. Epub 2020 Apr 2. J Endourol. 2020. PMID: 32098499
-
Perioperative, functional, and oncological outcomes of robotic vs. laparoscopic partial nephrectomy for complex renal tumors (RENAL score ≥7): an evidence-based analysis.Front Oncol. 2023 Jun 2;13:1195910. doi: 10.3389/fonc.2023.1195910. eCollection 2023. Front Oncol. 2023. PMID: 37664014 Free PMC article. Review.
-
Robotic versus laparoscopic partial nephrectomy for complex tumors: comparison of perioperative outcomes.Eur Urol. 2012 Jun;61(6):1257-62. doi: 10.1016/j.eururo.2012.03.012. Epub 2012 Mar 17. Eur Urol. 2012. PMID: 22464543
-
Nephrometry score-guided off-clamp laparoscopic partial nephrectomy: patient selection and short-time functional results.World J Surg Oncol. 2016 Jun 21;14(1):163. doi: 10.1186/s12957-016-0914-5. World J Surg Oncol. 2016. PMID: 27329038 Free PMC article.
-
Comparison of perioperative outcomes of robotic versus laparoscopic partial nephrectomy for complex renal tumors (RENAL nephrometry score of 7 or higher).Korean J Urol. 2014 Dec;55(12):808-13. doi: 10.4111/kju.2014.55.12.808. Epub 2014 Nov 26. Korean J Urol. 2014. PMID: 25512815 Free PMC article.
Cited by
-
Three-Dimensional Physical Model in Urologic Cancer.Front Surg. 2022 May 25;9:757337. doi: 10.3389/fsurg.2022.757337. eCollection 2022. Front Surg. 2022. PMID: 35693309 Free PMC article. Review.
-
Clinical implications of 3D printing technology in preoperative evaluation of partial nephrectomy.Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2022 Mar 28;47(3):328-333. doi: 10.11817/j.issn.1672-7347.2022.210586. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2022. PMID: 35545325 Free PMC article. Chinese, English.
-
Application of low-dose CT to the creation of 3D-printed kidney and perinephric tissue models for laparoscopic nephrectomy.Cancer Med. 2021 May;10(9):3077-3084. doi: 10.1002/cam4.3851. Epub 2021 Apr 2. Cancer Med. 2021. PMID: 33797861 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous