

Immune Checkpoint Inhibitors and Survival Outcomes in Brain Metastasis: A Time Series-Based Meta-Analysis
- PMID: 33194639
- PMCID: PMC7606910
- DOI: 10.3389/fonc.2020.564382
Immune Checkpoint Inhibitors and Survival Outcomes in Brain Metastasis: A Time Series-Based Meta-Analysis
Abstract
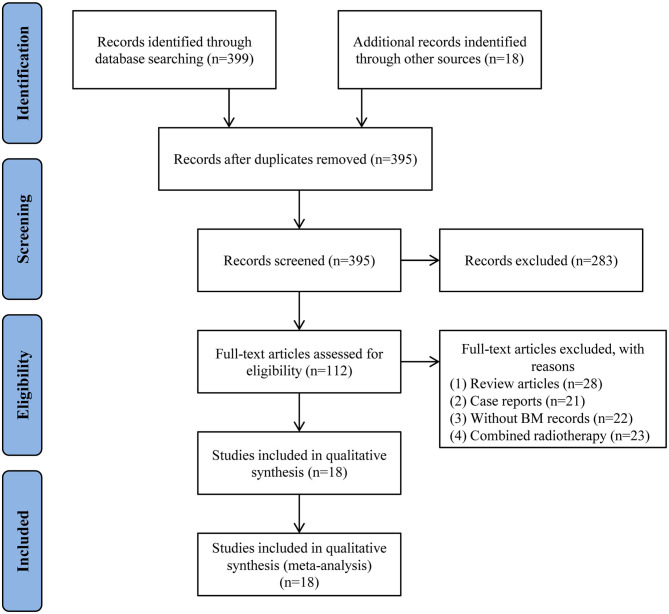
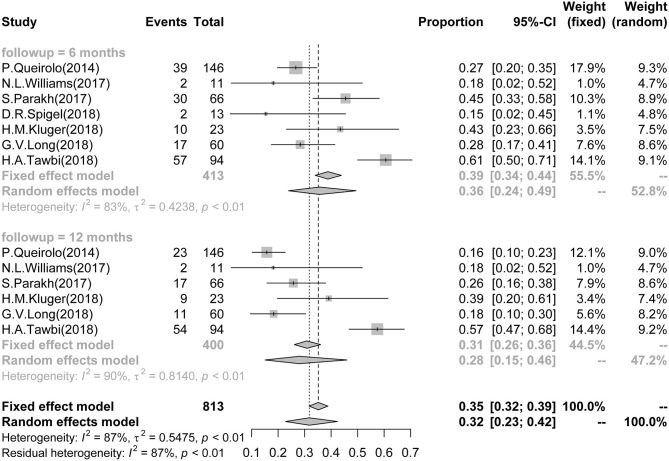
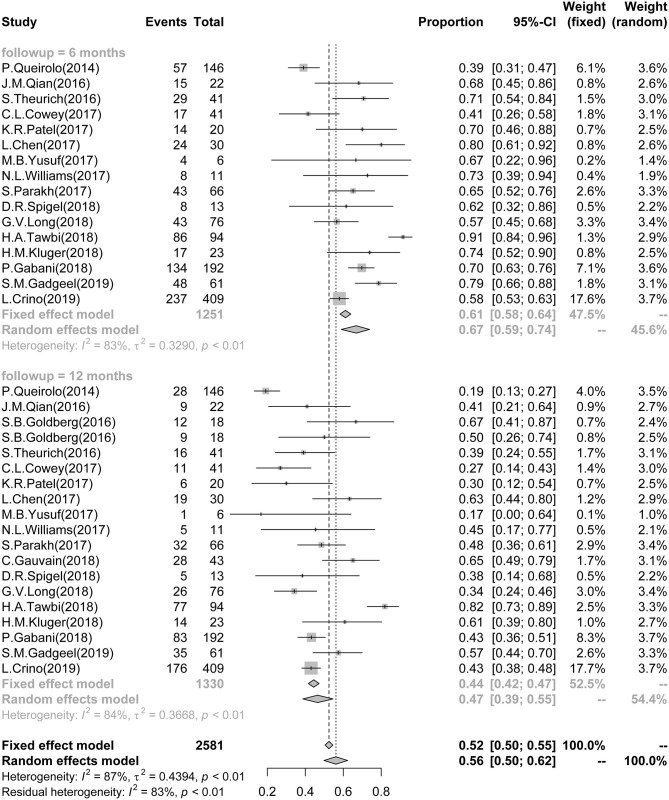
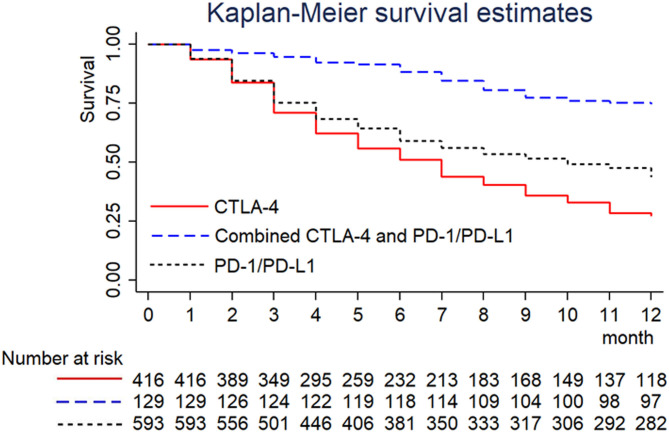
Immune checkpoint inhibitors (ICIs) have shown potential to improve the prognosis of patients with brain metastasis (BM) caused by advanced cancers. However, controversies still exist in regard to its survival benefits. In the present work, a time series-based meta-analysis based on the phase I/II/III trials and observational studies were performed to investigate the differences in mortality of ICI-treated BM patients. A number of public library databases, including MEDLINE, EMBASE, OVID, and COCHRANE, were systemically searched by March 2019. The quality of included studies was evaluated by the Newcastle-Ottawa Scale (NOS) scoring. Outcome measures here established were mortality and progression-free survival (PFS) at different follow-up endpoints. Survival rates and curve data were pooled for further analysis. To detect the data heterogeneity, subgroup analyses were conducted according to tumor and ICI types. Eighteen studies, 6 trials, and 12 controlled cohorts were assessed, involving a total of 1330 ICI-treated BM patients. The 6-month survival rate and PFS were 0.67 (95%CI: 0.59-0.74) and 0.36 (95%CI: 0.24-0.49), respectively. According to the tumor type (melanoma, NSCLC, and RCC), subgroup analyses indicated that melanoma presented the lowest survival rates among the three groups here selected. In regard to the type of ICIs, the anti-CTLA-4 combined with the anti-PD-1/PD-L1 showed the best survival outcome among these groups. The 12-month survival rate and PFS showed a consistent pattern of findings. In the long-term, the 24-month survival rate and PFS were 0.20 (95%CI: 0.12-0.31) and 0.18 (0.05-0.46) in BM patients. Hence, ICI therapy may be associated with an improved prognosis of BM patients. Nevertheless, current research presented a limited study design. Multicenter randomized trials may later assist in validating ICI-based therapies for a better outcome of BM patients.
Keywords: brain metastasis; immune checkpoint inhibitor; meta-analysis; prognosis; survival.
Copyright © 2020 Hu, Yu, Zheng, Zhang, Lin, Wang and Qiu.
Figures
References
-
- Balermpas P, Stera S, Müller von der Grün J, Loutfi-Krauss B, Forster MT, Wagner M, et al. Repeated in-field radiosurgery for locally recurrent brain metastases: feasibility, results and survival in a heavily treated patient cohort. PLoS One. (2018) 13:e0198692. 10.1371/journal.pone.0198692 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials