

Current Understanding of COVID-19 Clinical Course and Investigational Treatments
- PMID: 33195304
- PMCID: PMC7641603
- DOI: 10.3389/fmed.2020.555301
Current Understanding of COVID-19 Clinical Course and Investigational Treatments
Abstract
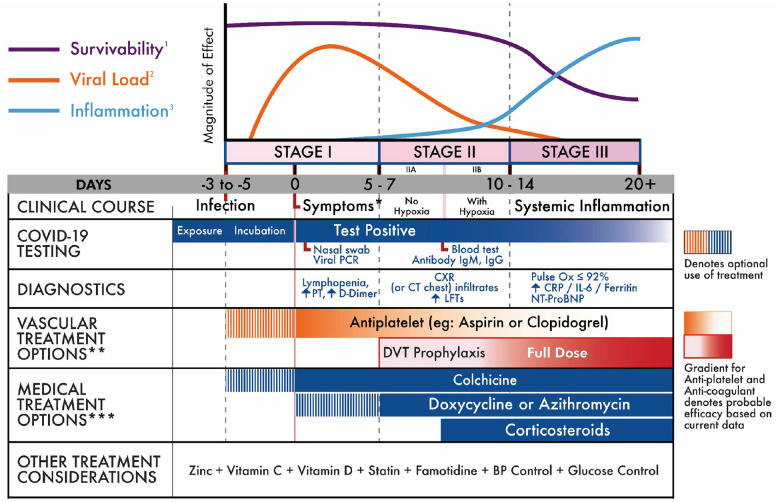
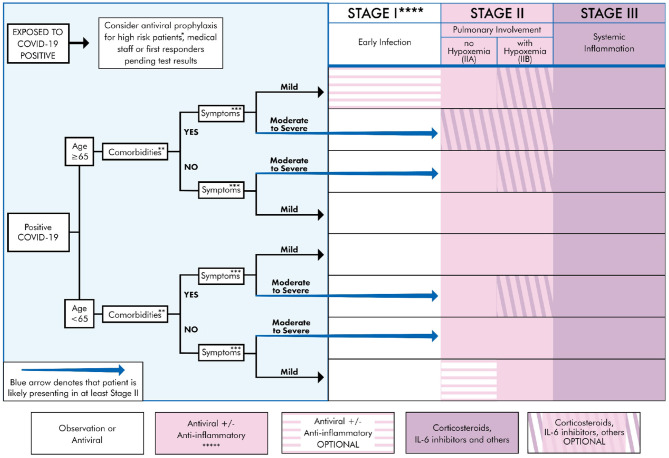
Importance: Currently, there is no unified framework linking disease progression to established viral levels, clinical tests, inflammatory markers, and investigational treatment options. Objective: It may take many weeks or months to establish a standard treatment approach. Given the growing morbidity and mortality with respect to COVID-19, this systemic review presents a treatment approach based on a thorough review of scholarly articles and clinical reports. Our focus is on staged progression, clinical algorithms, and individualized treatment. Evidence Review: We followed the protocol for a quality review article proposed by Heyn et al. (1). A literature search was conducted to find all relevant studies related to COVID-19. The search was conducted between April 1, 2020, and April 13, 2020, using the following electronic databases: PubMed (1809 to present); Google Scholar (1900 to present); MEDLINE (1946 to present), CINAHL (1937 to present); and Embase (1980 to present). The keywords used included COVID-19, 2019-nCov, SARS-CoV-2, SARS-CoV, and MERS-CoV, with terms such as efficacy, seroconversion, microbiology, pathophysiology, viral levels, inflammation, survivability, and treatment and pharmacology. No language restriction was placed on the search. Reference lists were manually scanned for additional studies. Findings: Of the articles found in the literature search, 70 were selected for inclusion in this study (67 cited in the body of the manuscript and 3 additional unique references in the Figures). The articles represent work from China, Japan, Taiwan, Vietnam, Rwanda, Israel, France, the United Kingdom, the Netherlands, Canada, and the United States. Most of the articles were cohort or case studies, but we also drew upon other information, including guidelines from hospitals and clinics instructing their staff on procedures to follow. In addition, we based some decisions on data collected by organizations such as the CDC, FDA, IHME, IDSA, and Worldometer. None of the case studies or cohort studies used a large number of participants. The largest group of participants numbered <500 and some case studies had fewer than 30 patients. However, the review of the literature revealed the need for individualized treatment protocols due to the variability of patient clinical presentation and survivability. A number of factors appear to influence mortality: the stage at which the patient first presented for care, pre-existing health conditions, age, and the viral load the patient carried. Conclusion and Relevance: COVID-19 can be divided into three distinct stages, beginning at the time of infection (Stage I), sometimes progressing to pulmonary involvement (Stage II, with or without hypoxemia), and less frequently to systemic inflammation (Stage III). In addition to modeling the stages of disease progression along with diagnostic testing, we have also created a treatment algorithm that considers age, comorbidities, clinical presentation, and disease progression to suggest drug classes or treatment modalities. This paper presents the first evidence-based recommendations for individualized treatment for COVID-19.
Keywords: COVID 19; clinical course; cover-19 testing; directed treatment; disease management; infectious disease.
Copyright © 2020 Aguilar, Hardigan, Mayi, Sider, Piotrkowski, Mehta, Dev, Seijo, Camargo, Andux, Hagen and Hernandez.
Figures


References
-
- Centers for Disease Control and Prevention Cases in U.S. 2020, August 19. Available online at: https://www.cdc.gov/coronavirus/2019-ncov/cases-updates/cases-in-us.html... (accessed August 19, 2020).
-
- The Institute for Health Metrics and Evaluation COVID-19. Available online at: https://covid19.healthdata.org/united-states-of-america (accessed August 20, 2020).
-
- Craven M, Liu L, Mysore M, Wilson M. COVID-19: Briefing Note. McKinsey and Company (2020). Available online at: https://www.mckinsey.com/~/media/McKinsey/Business%20Functions/Risk/Our%... (accessed April 6, 2020).
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous