

Laryngeal Injury and Upper Airway Symptoms After Endotracheal Intubation During Surgery: A Systematic Review and Meta-analysis
- PMID: 33196479
- PMCID: PMC7969363
- DOI: 10.1213/ANE.0000000000005276
Laryngeal Injury and Upper Airway Symptoms After Endotracheal Intubation During Surgery: A Systematic Review and Meta-analysis
Abstract
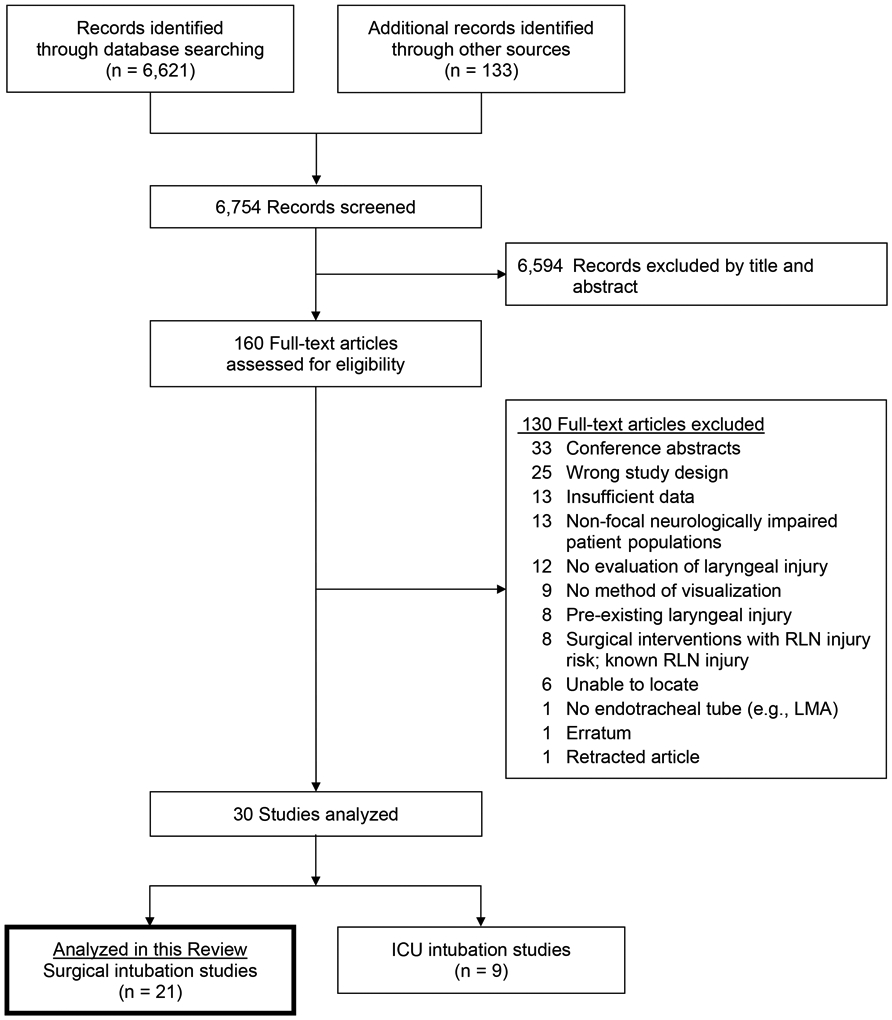
Laryngeal injury from intubation can substantially impact airway, voice, and swallowing, thus necessitating multidisciplinary interventions. The goals of this systematic review were (1) to review the types of laryngeal injuries and their patient-reported symptoms and clinical signs resulting from endotracheal intubation in patients intubated for surgeries and (2) to better understand the overall the frequency at which these injuries occur. We conducted a search of 4 online bibliographic databases (ie, PubMed, Embase, Cumulative Index of Nursing and Allied Health Literature [CINAHL], and The Cochrane Library) and ProQuest and Open Access Thesis Dissertations (OPTD) from database inception to September 2019 without restrictions for language. Studies that completed postextubation laryngeal examinations with visualization in adult patients who were endotracheally intubated for surgeries were included. We excluded (1) retrospective studies, (2) case studies, (3) preexisting laryngeal injury/disease, (4) patients with histories of or surgical interventions that risk injury to the recurrent laryngeal nerve, (5) conference abstracts, and (6) patient populations with nonfocal, neurological impairments that may impact voice and swallowing function, thus making it difficult to identify isolated postextubation laryngeal injury. Independent, double-data extraction, and risk of bias assessment followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and the Cochrane Collaboration's criteria. Twenty-one articles (1 cross-sectional, 3 cohort, 5 case series, 12 randomized controlled trials) representing 21 surgical studies containing 6140 patients met eligibility criteria. The mean patient age across studies reporting age was 49 (95% confidence interval [CI], 45-53) years with a mean intubation duration of 132 (95% CI, 106-159) minutes. Studies reported no injuries in 80% (95% CI, 69-88) of patients. All 21 studies presented on type of injury. Edema was the most frequently reported mild injury, with a prevalence of 9%-84%. Vocal fold hematomas were the most frequently reported moderate injury, with a prevalence of 4% (95% CI, 2-10). Severe injuries that include subluxation of the arytenoids and vocal fold paralysis are rare (<1%) outcomes. The most prevalent patient complaints postextubation were dysphagia (43%), pain (38%), coughing (32%), a sore throat (27%), and hoarseness (27%). Overall, laryngeal injury from short-duration surgical intubation is common and is most often mild. No uniform guidelines for laryngeal assessment postextubation from surgery are available and hoarseness is neither a good indicator of laryngeal injury or dysphagia. Protocolized screening for dysphonia and dysphagia postextubation may lead to improved identification of injury and, therefore, improved patient outcomes and reduced health care utilization.
Copyright © 2021 International Anesthesia Research Society.
Conflict of interest statement
Conflicts of Interest: See Disclosures at the end of the article.
Figures
References
-
- Durbin CG Jr., Bell CT, Shilling AM. Elective intubation. Respir Care. 2014;59(6):825–846; discussion 847-829. - PubMed
-
- Beckford NS, Mayo R, Wilkinson A 3rd, Tierney M. Effects of short-term endotracheal intubation on vocal function. Laryngoscope. 1990;100(4):331–336. - PubMed
-
- Hamdan AL, Sibai A, Rameh C, Kanazeh G. Short-term effects of endotracheal intubation on voice. J Voice. 2007;21(6):762–768. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
