

What Factors Predict Adverse Discharge Disposition in Patients Older Than 60 Years Undergoing Lower-extremity Surgery? The Adverse Discharge in Older Patients after Lower-extremity Surgery (ADELES) Risk Score
- PMID: 33196587
- PMCID: PMC7899493
- DOI: 10.1097/CORR.0000000000001532
What Factors Predict Adverse Discharge Disposition in Patients Older Than 60 Years Undergoing Lower-extremity Surgery? The Adverse Discharge in Older Patients after Lower-extremity Surgery (ADELES) Risk Score
Abstract
Background: Adverse discharge disposition, which is discharge to a long-term nursing home or skilled nursing facility is frequent and devastating in older patients after lower-extremity orthopaedic surgery. Predicting individual patient risk allows for preventive interventions to address modifiable risk factors and helps managing expectations. Despite a variety of risk prediction tools for perioperative morbidity in older patients, there is no tool available to predict successful recovery of a patient's ability to live independently in this highly vulnerable population.
Questions/purposes: In this study, we asked: (1) What factors predict adverse discharge disposition in patients older than 60 years after lower-extremity surgery? (2) Can a prediction instrument incorporating these factors be applied to another patient population with reasonable accuracy? (3) How does the instrument compare with other predictions scores that account for frailty, comorbidities, or procedural risk alone?
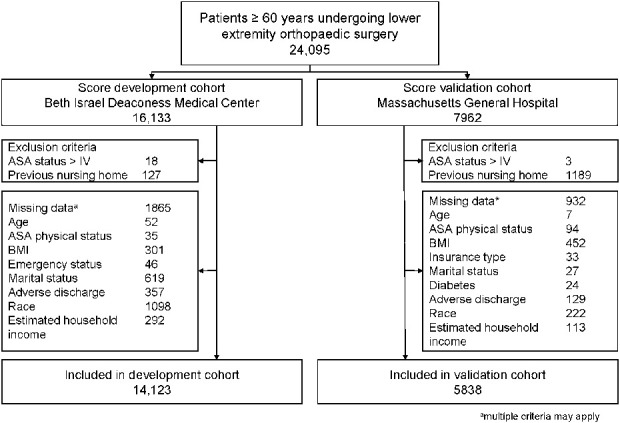
Methods: In this retrospective study at two competing New England university hospitals and Level 1 trauma centers with 673 and 1017 beds, respectively; 83% (19,961 of 24,095) of patients 60 years or older undergoing lower-extremity orthopaedic surgery were included. In all, 5% (1316 of 24,095) patients not living at home and 12% (2797 of 24,095) patients with missing data were excluded. All patients were living at home before surgery. The mean age was 72 ± 9 years, 60% (11,981 of 19,961) patients were female, 21% (4155 of 19,961) underwent fracture care, and 34% (6882 of 19,961) underwent elective joint replacements. Candidate predictors were tested in a multivariable logistic regression model for adverse discharge disposition in a development cohort of all 14,123 patients from the first hospital, and then included in a prediction instrument that was validated in all 5838 patients from the second hospital by calculating the area under the receiver operating characteristics curve (ROC-AUC).Thirty-eight percent (5360 of 14,262) of patients in the development cohort and 37% (2184 of 5910) of patients in the validation cohort had adverse discharge disposition. Score performance in predicting adverse discharge disposition was then compared with prediction scores considering frailty (modified Frailty Index-5 or mFI-5), comorbidities (Charlson Comorbidity Index or CCI), and procedural risks (Procedural Severity Scores for Morbidity and Mortality or PSS).
Results: After controlling for potential confounders like BMI, cardiac, renal and pulmonary disease, we found that the most prominent factors were age older than 90 years (10 points), hip or knee surgery (7 or 8 points), fracture management (6 points), dementia (5 points), unmarried status (3 points), federally provided insurance (2 points), and low estimated household income based on ZIP code (1 point). Higher score values indicate a higher risk of adverse discharge disposition. The score comprised 19 variables, including socioeconomic characteristics, surgical management, and comorbidities with a cutoff value of ≥ 23 points. Score performance yielded an ROC-AUC of 0.85 (95% confidence interval 0.84 to 0.85) in the development and 0.72 (95% CI 0.71 to 0.73) in the independent validation cohort, indicating excellent and good discriminative ability. Performance of the instrument in predicting adverse discharge in the validation cohort was superior to the mFI-5, CCI, and PSS (ROC-AUC 0.72 versus 0.58, 0.57, and 0.57, respectively).
Conclusion: The Adverse Discharge in Older Patients after Lower Extremity Surgery (ADELES) score predicts adverse discharge disposition after lower-extremity surgery, reflecting loss of the ability to live independently. Its discriminative ability is better than instruments that consider frailty, comorbidities, or procedural risk alone. The ADELES score identifies modifiable risk factors, including general anesthesia and prolonged preoperative hospitalization, and should be used to streamline patient and family expectation management and improve shared decision making. Future studies need to evaluate the score in community hospitals and in institutions with different rates of adverse discharge disposition and lower income. A non-commercial calculator can be accessed at www.adeles-score.org.
Level of evidence: Level III, diagnostic study.
Copyright © 2020 by the Association of Bone and Joint Surgeons.
Conflict of interest statement
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research® editors and board members are on file with the publication and can be viewed on request. Each remaining author certifies that neither he or she, nor any member of his or her immediate family, has funding or commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article.
Figures



Comment in
-
CORR Insights®: What Factors Predict Adverse Discharge Disposition in Patients Older Than 60 Years Undergoing Lower-extremity Surgery? The Adverse Discharge in Older Patients after Lower-extremity Surgery (ADELES) Risk Score.Clin Orthop Relat Res. 2021 Mar 1;479(3):558-560. doi: 10.1097/CORR.0000000000001575. Clin Orthop Relat Res. 2021. PMID: 33201023 Free PMC article. No abstract available.
References
-
- Bernstein DN Liu TC Winegar AL, et al. Evaluation of a preoperative optimization protocol for primary hip and knee arthroplasty patients. J Arthroplasty. 2018;33:3642–3648. - PubMed
-
- Bozic KJ, Wagie A, Naessens JM, Berry DJ, Rubash HE. Predictors of discharge to an inpatient extended care facility after total hip or knee arthroplasty. J Arthroplasty. 2006;21:151–156. - PubMed
-
- Cancio JM, Vela E, Santaeugènia S, Clèries M, Inzitari M, Ruiz D. Long-term impact of hip fracture on the use of healthcare resources: a population-based study. J Am Med Dir Assoc. 2019;20:456–461. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
