

Body mass index and risk of dying from a bloodstream infection: A Mendelian randomization study
- PMID: 33196656
- PMCID: PMC7668585
- DOI: 10.1371/journal.pmed.1003413
Body mass index and risk of dying from a bloodstream infection: A Mendelian randomization study
Abstract
Background: In observational studies of the general population, higher body mass index (BMI) has been associated with increased incidence of and mortality from bloodstream infection (BSI) and sepsis. On the other hand, higher BMI has been observed to be apparently protective among patients with infection and sepsis. We aimed to evaluate the causal association of BMI with risk of and mortality from BSI.
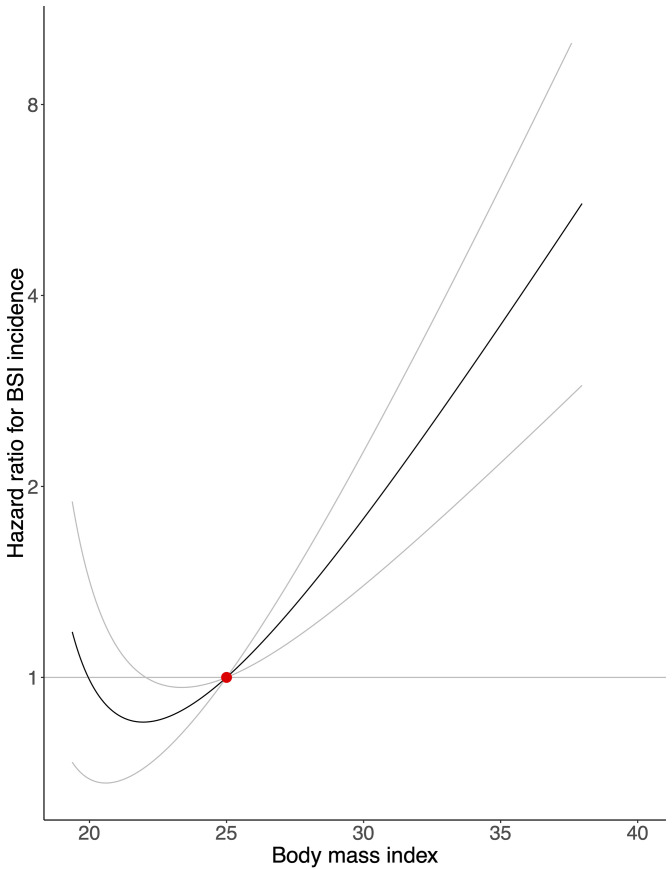
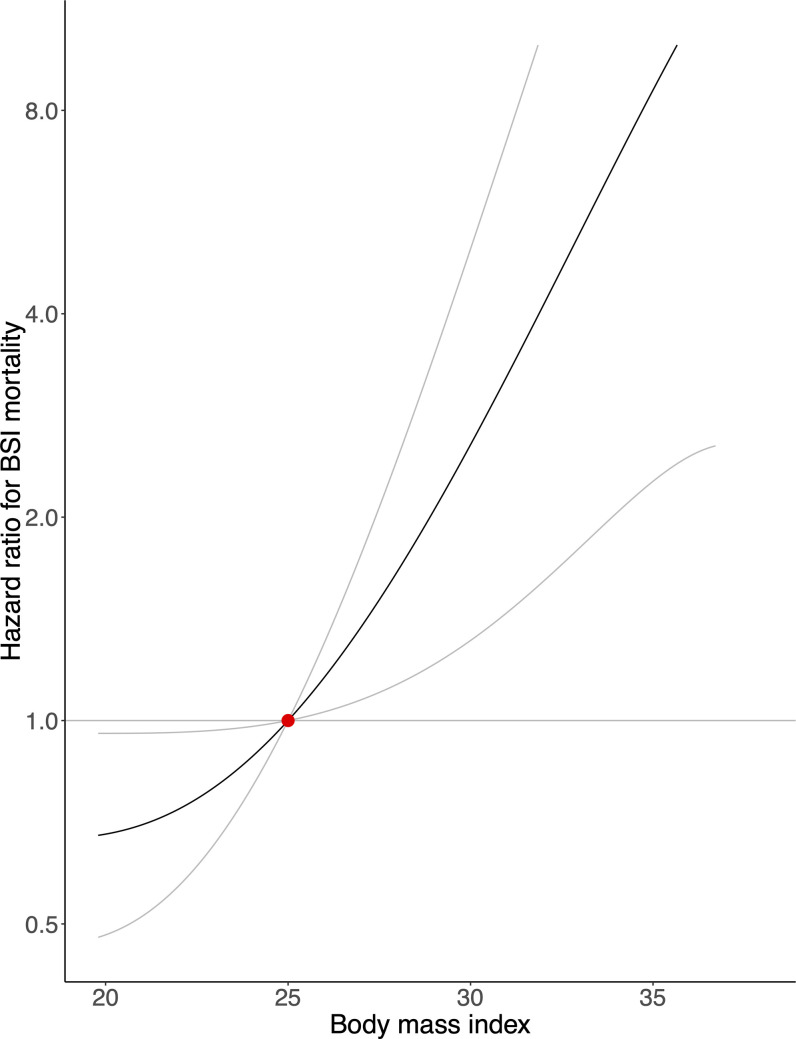
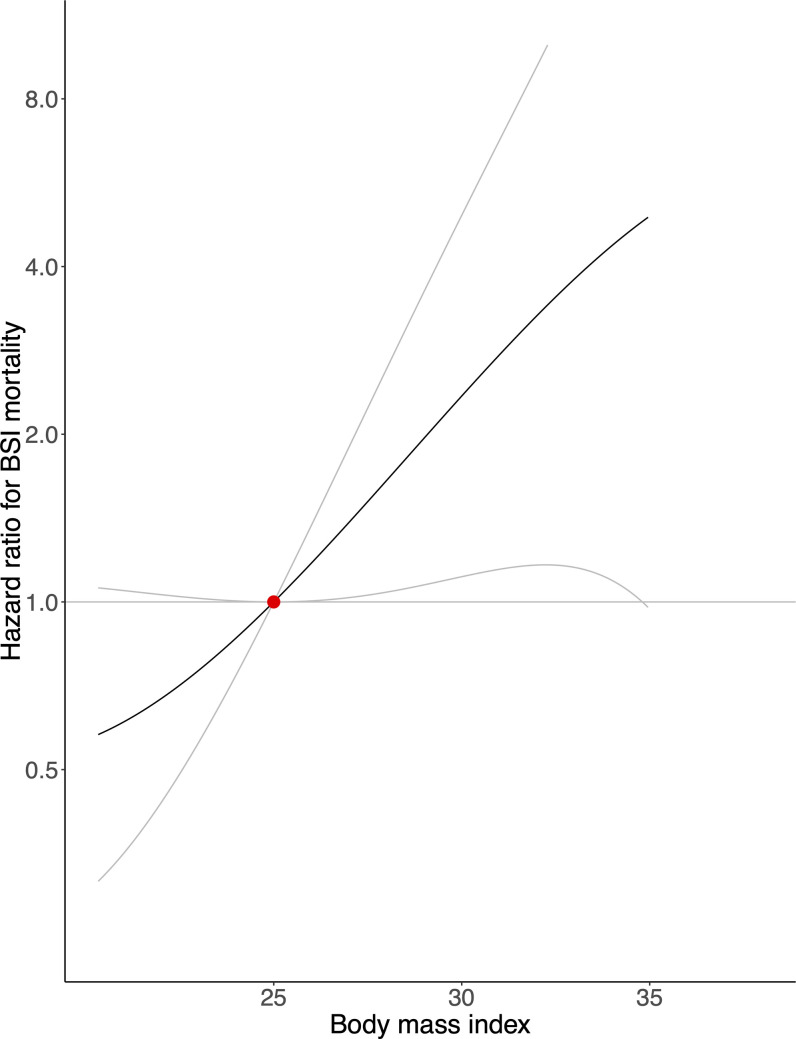
Methods and findings: We used a population-based cohort in Norway followed from 1995 to 2017 (the Trøndelag Health Study [HUNT]), and carried out linear and nonlinear Mendelian randomization analyses. Among 55,908 participants, the mean age at enrollment was 48.3 years, 26,324 (47.1%) were men, and mean BMI was 26.3 kg/m2. During a median 21 years of follow-up, 2,547 (4.6%) participants experienced a BSI, and 451 (0.8%) died from BSI. Compared with a genetically predicted BMI of 25 kg/m2, a genetically predicted BMI of 30 kg/m2 was associated with a hazard ratio for BSI incidence of 1.78 (95% CI: 1.40 to 2.27; p < 0.001) and for BSI mortality of 2.56 (95% CI: 1.31 to 4.99; p = 0.006) in the general population, and a hazard ratio for BSI mortality of 2.34 (95% CI: 1.11 to 4.94; p = 0.025) in an inverse-probability-weighted analysis of patients with BSI. Limitations of this study include a risk of pleiotropic effects that may affect causal inference, and that only participants of European ancestry were considered.
Conclusions: Supportive of a causal relationship, genetically predicted BMI was positively associated with BSI incidence and mortality in this cohort. Our findings contradict the "obesity paradox," where previous traditional epidemiological studies have found increased BMI to be apparently protective in terms of mortality for patients with BSI or sepsis.
Conflict of interest statement
I have read the journal's policy and the authors of this manuscript have the following competing interests: SB is a paid statistical reviewer for PLOS Medicine. HCP has current or prior grant funding from the NIH, AHRQ, and the US Department of Veterans Affairs. The other authors have declared that no competing interests exist.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
