

A Bayesian phase 2 model based adaptive design to optimise antivenom dosing: Application to a dose-finding trial for a novel Russell's viper antivenom in Myanmar
- PMID: 33196672
- PMCID: PMC7704047
- DOI: 10.1371/journal.pntd.0008109
A Bayesian phase 2 model based adaptive design to optimise antivenom dosing: Application to a dose-finding trial for a novel Russell's viper antivenom in Myanmar
Abstract
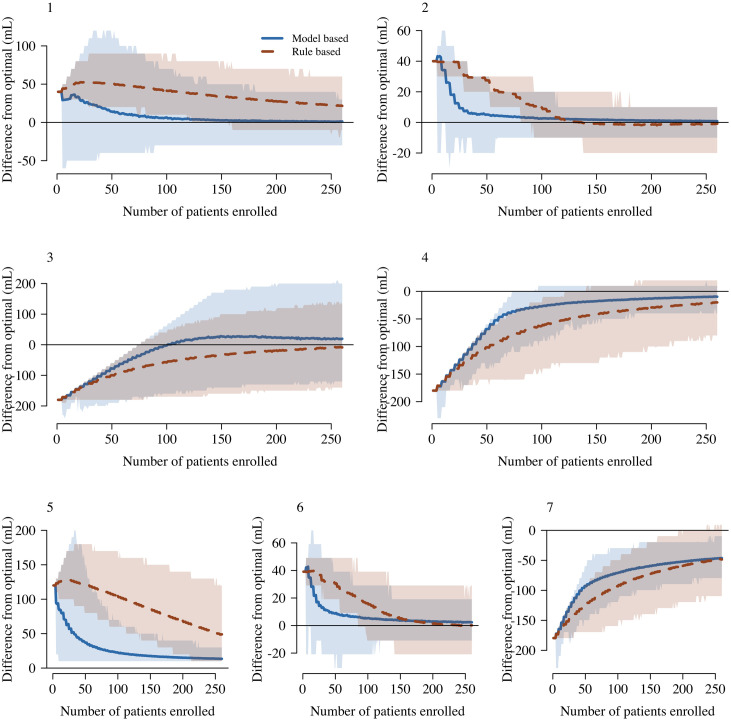
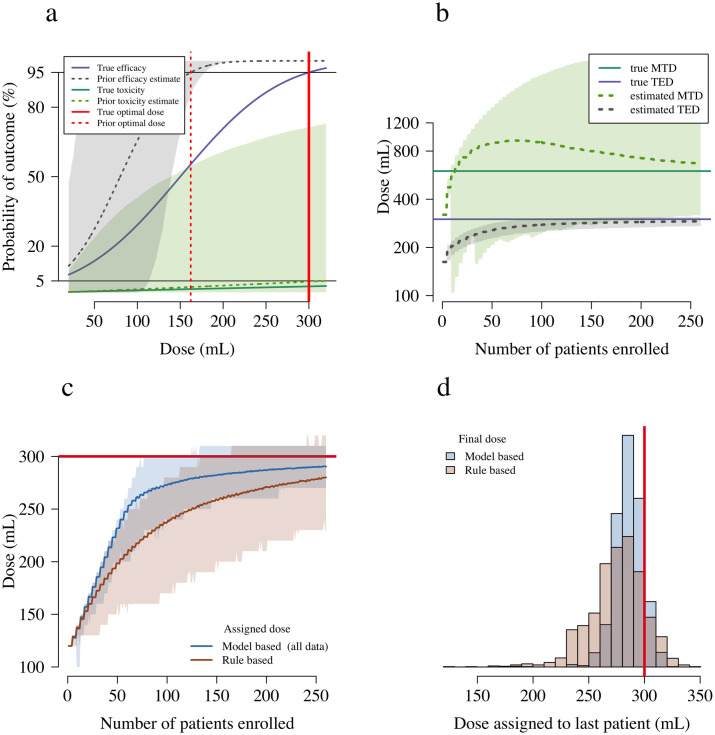
For most antivenoms there is little information from clinical studies to infer the relationship between dose and efficacy or dose and toxicity. Antivenom dose-finding studies usually recruit too few patients (e.g. fewer than 20) relative to clinically significant event rates (e.g. 5%). Model based adaptive dose-finding studies make efficient use of accrued patient data by using information across dosing levels, and converge rapidly to the contextually defined 'optimal dose'. Adequate sample sizes for adaptive dose-finding trials can be determined by simulation. We propose a model based, Bayesian phase 2 type, adaptive clinical trial design for the characterisation of optimal initial antivenom doses in contexts where both efficacy and toxicity are measured as binary endpoints. This design is illustrated in the context of dose-finding for Daboia siamensis (Eastern Russell's viper) envenoming in Myanmar. The design formalises the optimal initial dose of antivenom as the dose closest to that giving a pre-specified desired efficacy, but resulting in less than a pre-specified maximum toxicity. For Daboia siamensis envenoming, efficacy is defined as the restoration of blood coagulability within six hours, and toxicity is defined as anaphylaxis. Comprehensive simulation studies compared the expected behaviour of the model based design to a simpler rule based design (a modified '3+3' design). The model based design can identify an optimal dose after fewer patients relative to the rule based design. Open source code for the simulations is made available in order to determine adequate sample sizes for future adaptive snakebite trials. Antivenom dose-finding trials would benefit from using standard model based adaptive designs. Dose-finding trials where rare events (e.g. 5% occurrence) are of clinical importance necessitate larger sample sizes than current practice. We will apply the model based design to determine a safe and efficacious dose for a novel lyophilised antivenom to treat Daboia siamensis envenoming in Myanmar.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

Similar articles
-
Evaluation of the geographical utility of Eastern Russell's viper (Daboia siamensis) antivenom from Thailand and an assessment of its protective effects against venom-induced nephrotoxicity.PLoS Negl Trop Dis. 2019 Oct 23;13(10):e0007338. doi: 10.1371/journal.pntd.0007338. eCollection 2019 Oct. PLoS Negl Trop Dis. 2019. PMID: 31644526 Free PMC article.
-
An open, randomized comparative trial of two antivenoms for the treatment of envenoming by Sri Lankan Russell's viper (Daboia russelii russelii).Trans R Soc Trop Med Hyg. 2001 Jan-Feb;95(1):74-80. doi: 10.1016/s0035-9203(01)90339-6. Trans R Soc Trop Med Hyg. 2001. PMID: 11280073 Clinical Trial.
-
A randomized controlled trial of fresh frozen plasma for coagulopathy in Russell's viper (Daboia russelii) envenoming.J Thromb Haemost. 2017 Apr;15(4):645-654. doi: 10.1111/jth.13628. Epub 2017 Feb 16. J Thromb Haemost. 2017. PMID: 28106331 Free PMC article. Clinical Trial.
-
Snakebite associated thrombotic microangiopathy: a systematic review of clinical features, outcomes, and evidence for interventions including plasmapheresis.PLoS Negl Trop Dis. 2020 Dec 8;14(12):e0008936. doi: 10.1371/journal.pntd.0008936. eCollection 2020 Dec. PLoS Negl Trop Dis. 2020. PMID: 33290400 Free PMC article.
-
Antivenom therapy of carpet viper (Echis ocellatus) envenoming: effectiveness and strategies for delivery in West Africa.Toxicon. 2013 Jul;69:82-9. doi: 10.1016/j.toxicon.2013.01.002. Epub 2013 Jan 20. Toxicon. 2013. PMID: 23339853 Review.
Cited by
-
Managing snakebite.BMJ. 2022 Jan 7;376:e057926. doi: 10.1136/bmj-2020-057926. BMJ. 2022. PMID: 34996773 Free PMC article. Review. No abstract available.
-
Access to antivenoms in the developing world: A multidisciplinary analysis.Toxicon X. 2021 Oct 26;12:100086. doi: 10.1016/j.toxcx.2021.100086. eCollection 2021 Nov. Toxicon X. 2021. PMID: 34786555 Free PMC article.
-
Clinical management of snakebite envenoming: Future perspectives.Toxicon X. 2021 Aug 8;11:100079. doi: 10.1016/j.toxcx.2021.100079. eCollection 2021 Sep. Toxicon X. 2021. PMID: 34430847 Free PMC article.
References
-
- Kasturiratne A, Wickremasinghe AR, De Silva N, Gunawardena NK, Pathmeswaran A, Premaratna R, et al. The global burden of snakebite: A literature analysis and modelling based on regional estimates of envenoming and deaths. PLoS Medicine. 2008;5(11):1591–1604. 10.1371/journal.pmed.0050218 - DOI - PMC - PubMed
-
- Gutiérrez JM, Calvete JJ, Habib AG, Harrison RA, Williams DJ, Warrell DA. Snakebite envenoming. Nature Reviews. 2017;3:17063 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
