

Changes in Health Care Use and Outcomes After Turnover in Primary Care
- PMID: 33196767
- PMCID: PMC7670398
- DOI: 10.1001/jamainternmed.2020.6288
Changes in Health Care Use and Outcomes After Turnover in Primary Care
Abstract
Importance: Disruptions of continuity of care may harm patient outcomes, but existing studies of continuity disruption are limited by an inability to separate the association of continuity disruption from that of other physician-related factors.
Objectives: To examine changes in health care use and outcomes among patients whose primary care physician (PCP) exited the workforce and to directly measure the association of this primary care turnover with patients' health care use and outcomes.
Design, setting, and participants: This cohort study used nationally representative Medicare billing claims for a random sample of 359 470 Medicare fee-for-service beneficiaries with at least 1 PCP evaluation and management visit from January 1, 2008, to December 31, 2017. Primary care physicians who stopped practicing were identified and matched with PCPs who remained in practice. A difference-in-differences analysis compared health care use and clinical outcomes for patients who did lose PCPs with those who did not lose PCPs using subgroup analyses by practice size. Subgroup analyses were done on visits from January 1, 2008, to December 31, 2017.
Exposure: Patients' loss of a PCP.
Main outcomes and measures: Primary care, specialty care, urgent care, emergency department, and inpatient visits, as well as overall spending for patients, were the primary outcomes. Receipt of appropriate preventive care and prescription fills were also examined.
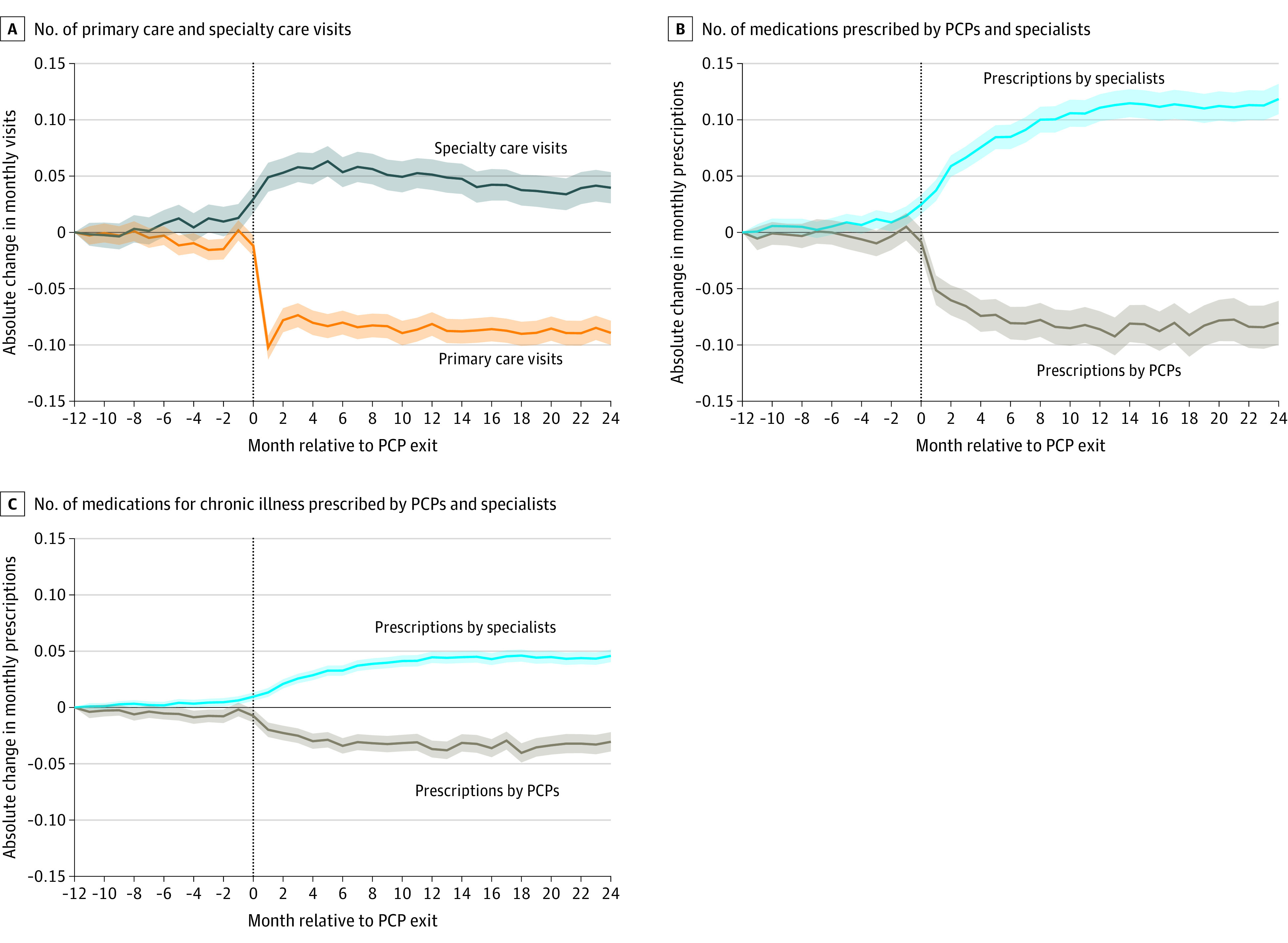
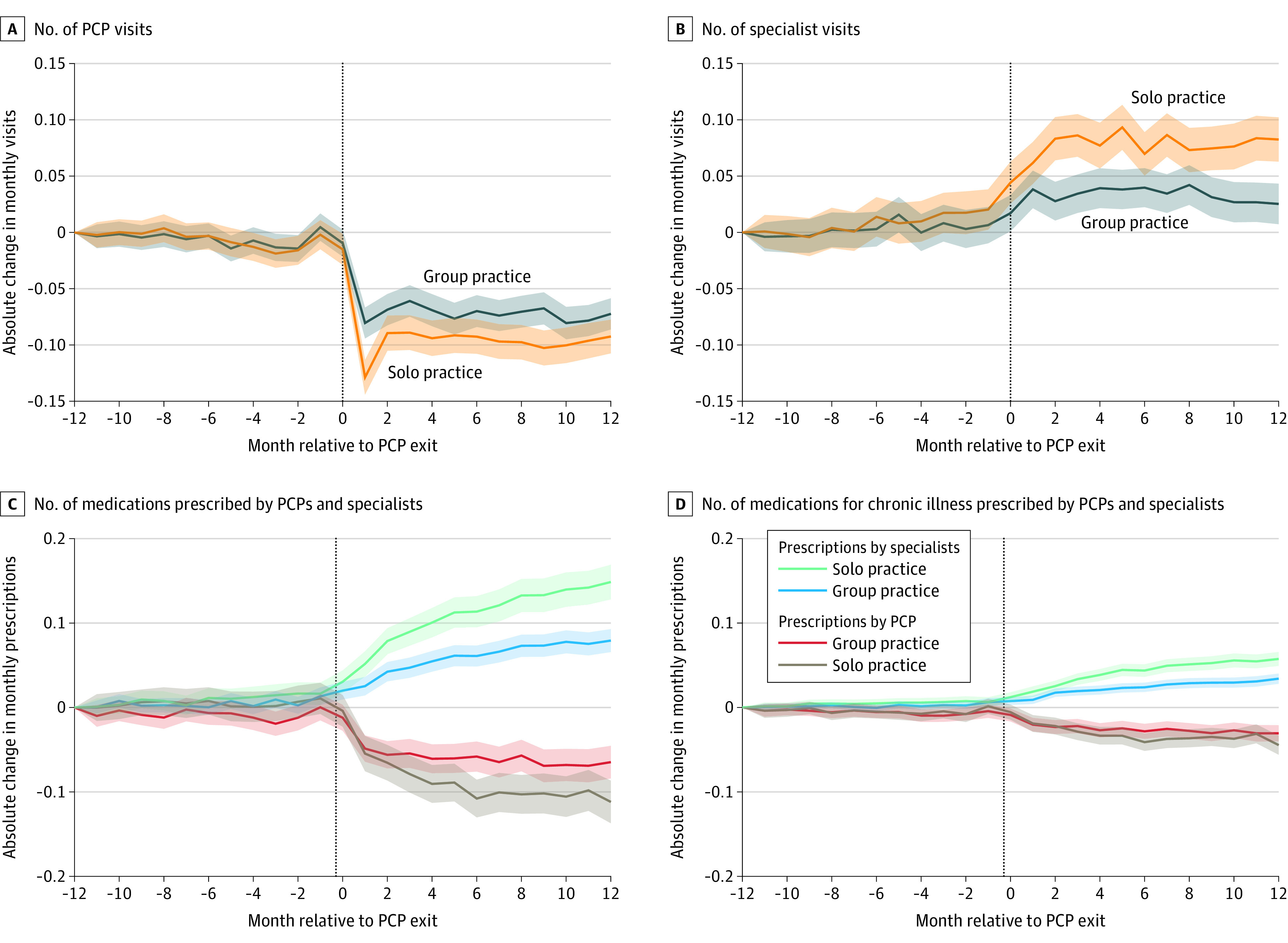
Results: During the study period, 9491 of 90 953 PCPs (10.4%) exited Medicare. We matched 169 870 beneficiaries whose PCP exited (37.2% women; mean [SD] age, 71.4 [6.1] years) with 189 600 beneficiaries whose PCP did not exit (36.9% women; mean [SD] age, 72.0 [5.0] years). The year after PCP exit, beneficiaries whose PCP exited had 18.4% (95% CI, -19.8% to -16.9%) fewer primary care visits and 6.2% (95% CI, 5.4%-7.0%) more specialty care visits compared with beneficiaries who did not lose a PCP. This outcome persisted 2 years after PCP exit. Beneficiaries whose PCP exited also had 17.8% (95% CI, 6.0%-29.7%) more urgent care visits, 3.1% (95% CI, 1.6%-4.6%) more emergency department visits, and greater spending ($189 [95% CI, $30-$347]) per beneficiary-year after PCP exit. These shifts were most pronounced for patients of exiting PCPs in solo practice, whose beneficiaries had 21.5% (95% CI, -23.8% to -19.3%) fewer primary care visits, 8.8% (95% CI, 7.6%-10.0%) more specialty care visits, 4.4% more emergency department visits (95% CI, 2.1%-6.7%), and $260 (95% CI, $12-$509) in increased spending.
Conclusions and relevance: Loss of a PCP was associated with lower use of primary care and increased use of specialty, urgent, and emergency care among Medicare beneficiaries. Interrupting primary care relationships may negatively impact health outcomes and future engagement with primary care.
Conflict of interest statement
Figures
References
-
- Mainous AG III, Kern D, Hainer B, Kneuper-Hall R, Stephens J, Geesey ME. The relationship between continuity of care and trust with stage of cancer at diagnosis. Fam Med. 2004;36(1):35-39. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
