

Clinical Effects of Balanced Crystalloids vs Saline in Adults With Diabetic Ketoacidosis: A Subgroup Analysis of Cluster Randomized Clinical Trials
- PMID: 33196806
- PMCID: PMC7670314
- DOI: 10.1001/jamanetworkopen.2020.24596
Clinical Effects of Balanced Crystalloids vs Saline in Adults With Diabetic Ketoacidosis: A Subgroup Analysis of Cluster Randomized Clinical Trials
Abstract
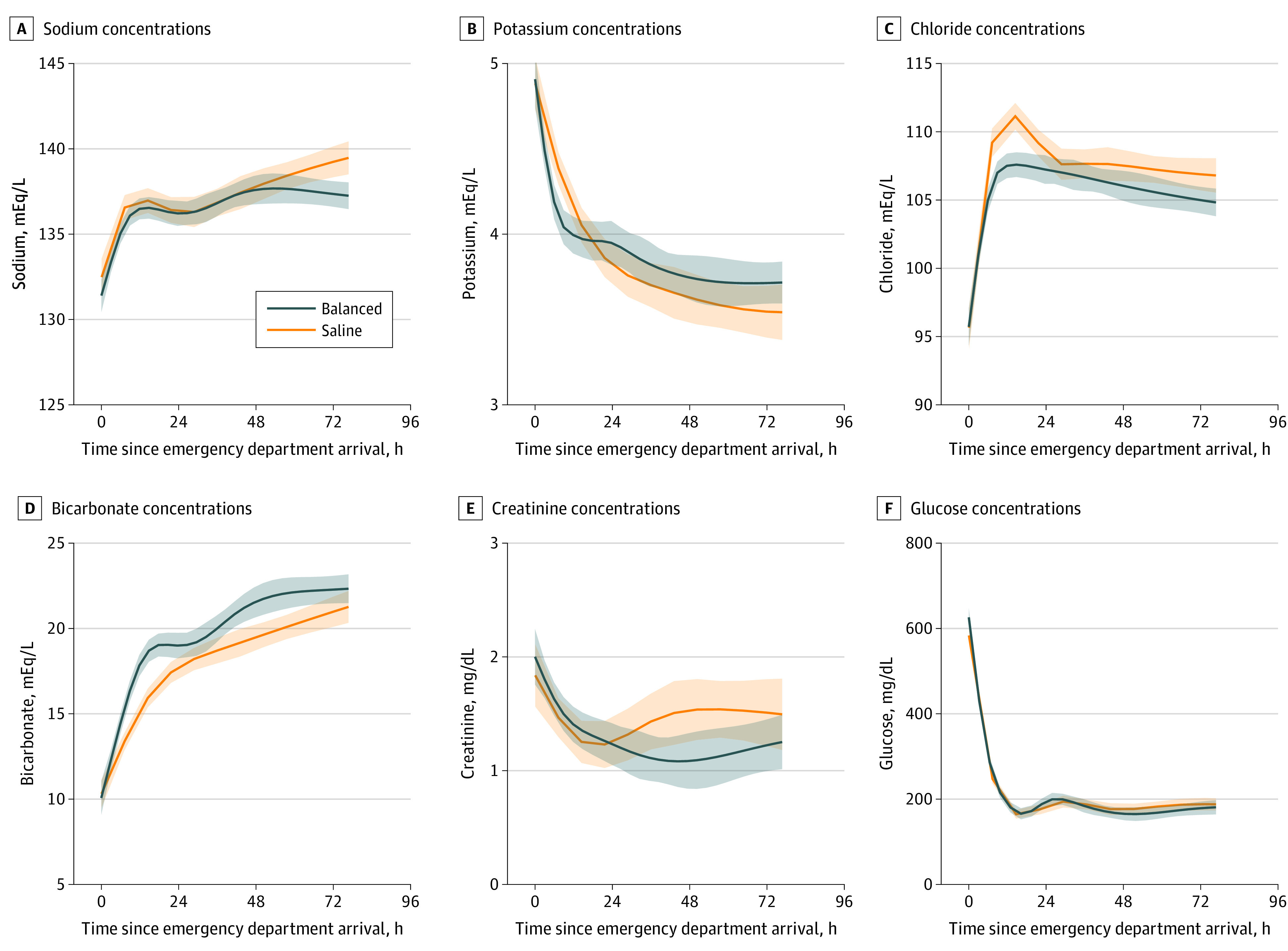
Importance: Saline (0.9% sodium chloride), the fluid most commonly used to treat diabetic ketoacidosis (DKA), can cause hyperchloremic metabolic acidosis. Balanced crystalloids, an alternative class of fluids for volume expansion, do not cause acidosis and, therefore, may lead to faster resolution of DKA than saline.
Objective: To compare the clinical effects of balanced crystalloids with the clinical effects of saline for the acute treatment of adults with DKA.
Design, setting, and participants: This study was a subgroup analysis of adults with DKA in 2 previously reported companion trials-Saline Against Lactated Ringer's or Plasma-Lyte in the Emergency Department (SALT-ED) and the Isotonic Solutions and Major Adverse Renal Events Trial (SMART). These trials, conducted between January 2016 and March 2017 in an academic medical center in the US, were pragmatic, multiple-crossover, cluster, randomized clinical trials comparing balanced crystalloids vs saline in emergency department (ED) and intensive care unit (ICU) patients. This study included adults who presented to the ED with DKA, defined as a clinical diagnosis of DKA, plasma glucose greater than 250 mg/dL, plasma bicarbonate less than or equal to 18 mmol/L, and anion gap greater than 10 mmol/L. Data analysis was performed from January to April 2020.
Interventions: Balanced crystalloids (clinician's choice of Ringer lactate solution or Plasma-Lyte A solution) vs saline for fluid administration in the ED and ICU according to the same cluster-randomized multiple-crossover schedule.
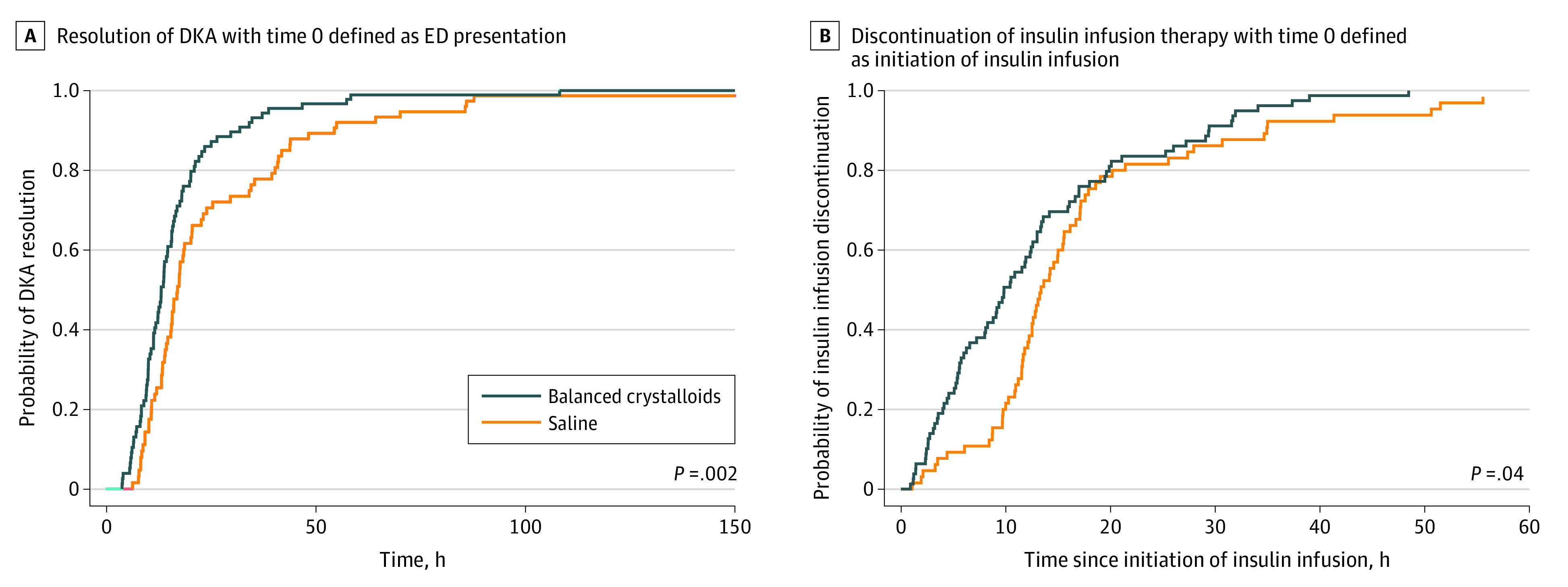
Main outcomes and measures: The primary outcome was time between ED presentation and DKA resolution, as defined by American Diabetes Association criteria. The secondary outcome was time between initiation and discontinuation of continuous insulin infusion.
Results: Among 172 adults included in this secondary analysis of cluster trials, 94 were assigned to balanced crystalloids and 78 to saline. The median (interquartile range [IQR]) age was 29 (24-45) years, and 90 (52.3%) were women. The median (IQR) volume of isotonic fluid administered in the ED and ICU was 4478 (3000-6372) mL. Cumulative incidence analysis revealed shorter time to DKA resolution in the balanced crystalloids group (median time to resolution: 13.0 hours; IQR: 9.5-18.8 hours) than the saline group (median: 16.9 hours; IQR: 11.9-34.5 hours) (adjusted hazard ratio [aHR] = 1.68; 95% CI, 1.18-2.38; P = .004). Cumulative incidence analysis also revealed shorter time to insulin infusion discontinuation in the balanced crystalloids group (median: 9.8 hours; IQR: 5.1-17.0 hours) than the saline group (median: 13.4 hours; IQR: 11.0-17.9 hours) (aHR = 1.45; 95% CI, 1.03-2.03; P = .03).
Conclusions and relevance: In this secondary analysis of 2 cluster randomized clinical trials, compared with saline, treatment with balanced crystalloids resulted in more rapid resolution of DKA, suggesting that balanced crystalloids may be preferred over saline for acute management of adults with DKA.
Trial registration: ClinicalTrials.gov Identifiers: NCT02614040; NCT02444988.
Conflict of interest statement
Figures
References
-
- Joint British Diabetes Societies Inpatient Care Group The management of diabetic ketoacidosis in adults, 2nd edition. Published 2013. Accessed December 3, 2018. https://www.diabetes.org.uk/resources-s3/2017-09/Management-of-DKA-24101...
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
