

Patient Adherence to Screening for Lung Cancer in the US: A Systematic Review and Meta-analysis
- PMID: 33196807
- PMCID: PMC7670313
- DOI: 10.1001/jamanetworkopen.2020.25102
Patient Adherence to Screening for Lung Cancer in the US: A Systematic Review and Meta-analysis
Abstract
Importance: To be effective in reducing deaths from lung cancer among high-risk current and former smokers, screening with low-dose computed tomography must be performed periodically.
Objective: To examine lung cancer screening (LCS) adherence rates reported in the US, patient characteristics associated with adherence, and diagnostic testing rates after screening.
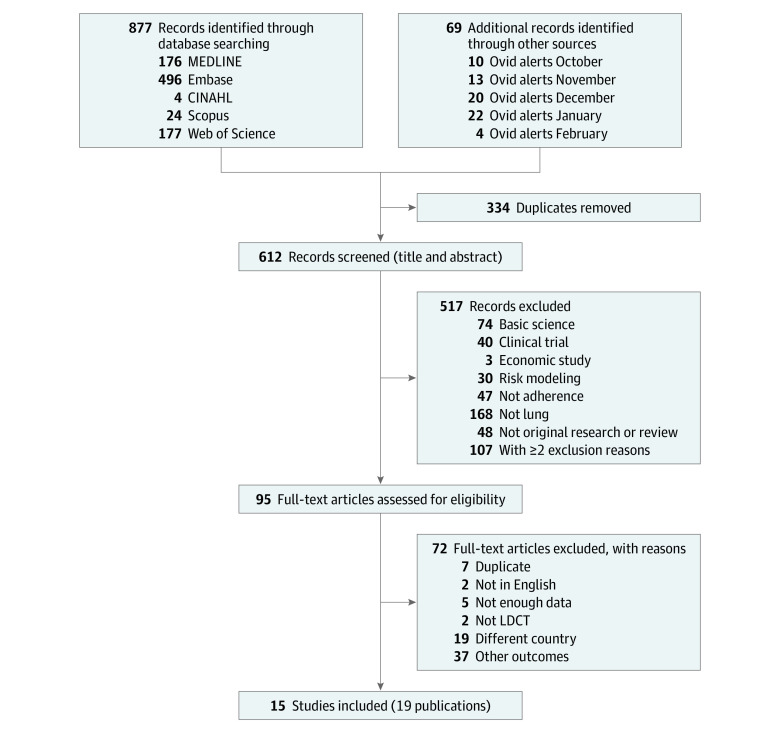
Data sources: Five electronic databases (MEDLINE, Embase, Scopus, CINAHL, and Web of Science) were searched for articles published in the English language from January 1, 2011, through February 28, 2020.
Study selection: Two reviewers independently selected prospective and retrospective cohort studies from 95 potentially relevant studies reporting patient LCS adherence.
Data extraction and synthesis: Quality appraisal and data extraction were performed independently by 2 reviewers using the Newcastle-Ottawa Scale for quality assessment. A random-effects model meta-analysis was conducted when at least 2 studies reported on the same outcome. Reporting followed the Preferred Reporting Items for Systematic Review and Meta-analyses (PRISMA) guideline.
Main outcomes and measures: The primary outcome was LCS adherence after a baseline screening. Secondary measures were the patient characteristics associated with adherence and the rate of diagnostic testing after screening.
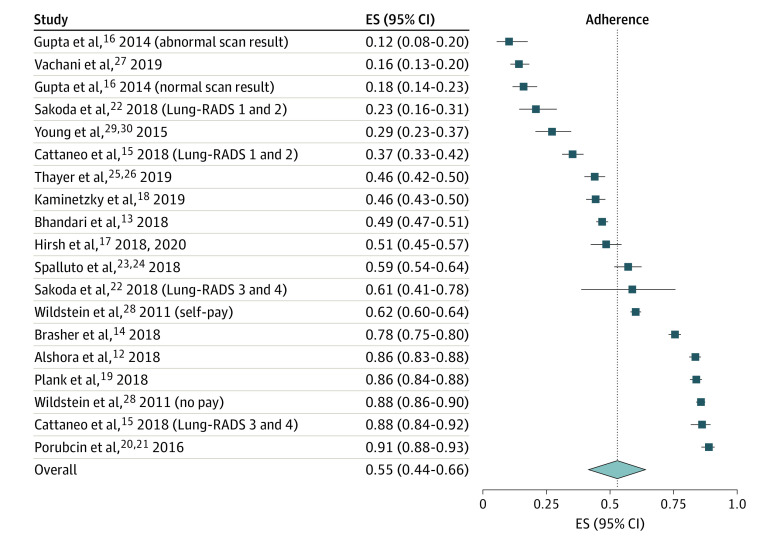
Results: Fifteen studies with a total of 16 863 individuals were included in this systematic review and meta-analysis. The pooled LCS adherence rate across all follow-up periods (range, 12-36 months) was 55% (95% CI, 44%-66%). Regarding patient characteristics associated with adherence rates, current smokers were less likely to adhere to LCS than former smokers (odds ratio [OR], 0.70; 95% CI, 0.62-0.80); White patients were more likely to adhere to LCS than patients of races other than White (OR, 2.0; 95% CI, 1.6-2.6); people 65 to 73 years of age were more likely to adhere to LCS than people 50 to 64 years of age (OR, 1.4; 95% CI, 1.0-1.9); and completion of 4 or more years of college was also associated with increased adherence compared with people not completing college (OR, 1.5; 95% CI, 1.1-2.1). Evidence was insufficient to evaluate diagnostic testing rates after abnormal screening scan results. The main source of variation was attributable to the eligibility criteria for screening used across studies.
Conclusions and relevance: In this study, the pooled LCS adherence rate after a baseline screening was far lower than those observed in large randomized clinical trials of screening. Interventions to promote adherence to screening should prioritize current smokers and smokers from minority populations.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
