

Opioid Prescribing and Opioid Risk Mitigation Strategies in the Veterans Health Administration
- PMID: 33196968
- PMCID: PMC7728840
- DOI: 10.1007/s11606-020-06258-3
Opioid Prescribing and Opioid Risk Mitigation Strategies in the Veterans Health Administration
Abstract
Introduction: The Veterans Health Administration (VHA) has taken a multifaceted approach to addressing opioid safety and promoting system-wide opioid stewardship.
Aim: To provide a comprehensive evaluation of current opioid prescribing practices and implementation of risk mitigation strategies in VHA.
Setting: VHA is the largest integrated health care system in the United States.
Program description: VHA prescribing data in conjunction with implementation of opioid risk mitigation strategies are routinely tracked and reviewed by VHA's Pharmacy Benefits Management Services (including Academic Detailing Service) and the Pain Management Program Office. Additional data are derived from the Partnered Evidence-Based Policy Resource Center (PEPReC) and from a 2019 survey of interdisciplinary pain management teams at VHA facilities. Prescribing data are reported quarterly until first quarter fiscal year 2020 (Q1FY2020), ending December 31, 2019.
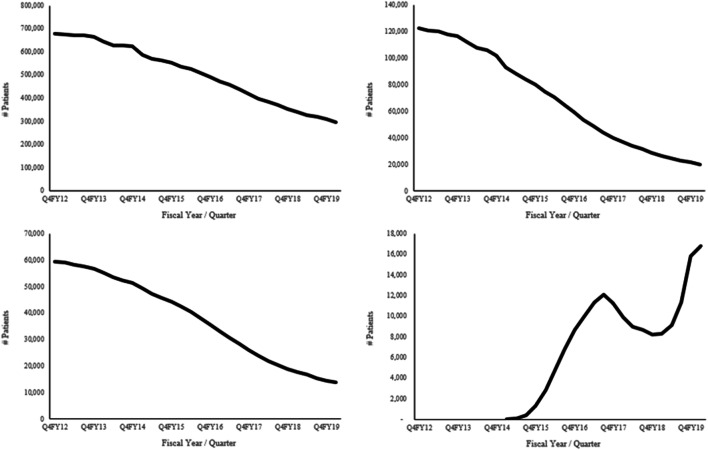
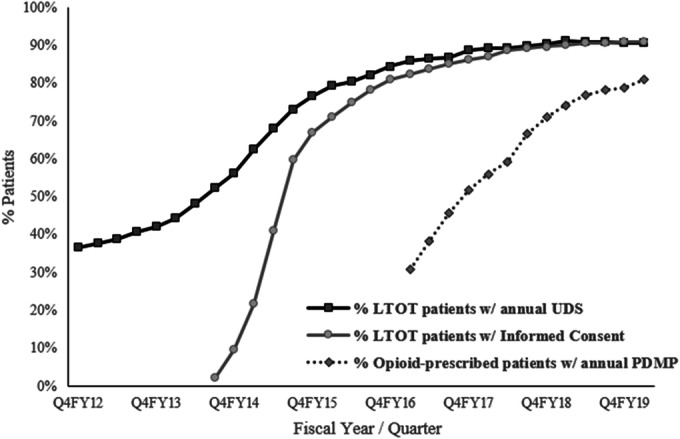
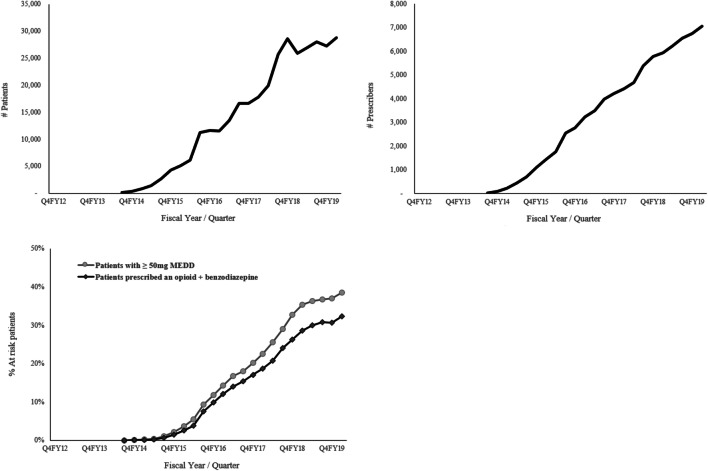
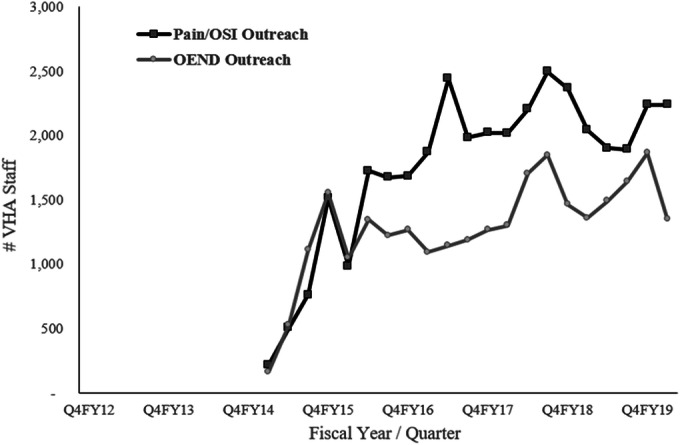
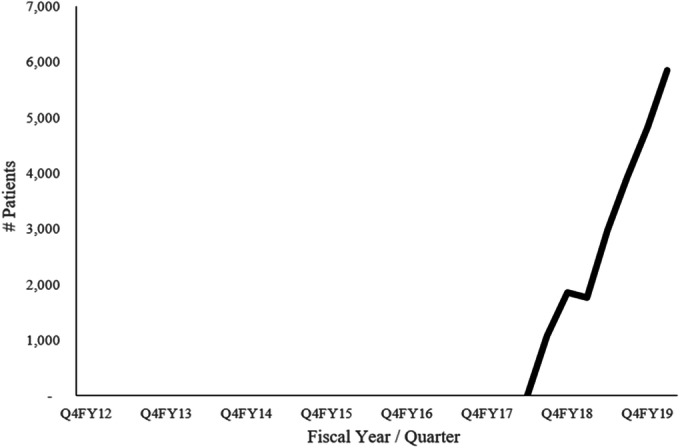
Program evaluation: VHA opioid dispensing peaked in 2012 with 679,376 Veterans receiving an opioid prescription, and when including tramadol, in 2013 with 869,956 Veterans. Since 2012, the number of Veterans dispensed an opioid decreased 56% and co-prescribed opioid/benzodiazepine decreased 83%. Veterans with high-dose opioids (≥ 100 mg morphine equivalent daily dose) decreased 77%. In Q1FY2020, among Veterans on long-term opioid therapy (LTOT), 91.1% had written informed consent, 90.8% had a urine drug screen, and 89.0% had a prescription drug monitoring program query. Naloxone was issued to 217,469 Veterans and resulted in > 1,000 documented overdose reversals. In 2019, interdisciplinary pain management teams were fully designated at 68%, partially designated at 28%, and not available at 4% of 140 VA parent facilities. Fifty percent of Veterans on opioids at very high risk for overdose/suicide received interdisciplinary team reviews.
Implications: VHA clinicians have greatly reduced their volume of opioid prescribing for pain management and expanded implementation of opioid risk mitigation strategies.
Impacts: VHA's integrated health care system provides a model for opioid stewardship and interdisciplinary pain care.
Keywords: VHA; academic detailing; opioid epidemic; opioids; pain management.
Conflict of interest statement
The authors declare that they do not have a conflict of interest.
Figures
References
-
- Carey E, Leonard C. Caring for Veterans Reporting Chronic Pain: Provider experiences and trends in the prevalence of chronic pain. Available at: https://www.hsrd.research.va.gov/for_researchers/cyber_seminars/archives.... Accessed June 25, 2020.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
