

doi: 10.1164/rccm.202006-2394PP.
The Epidemiological Importance of Subclinical Tuberculosis. A Critical Reappraisal
Affiliations
- PMID: 33197210
- PMCID: PMC7874405
- DOI: 10.1164/rccm.202006-2394PP
Item in Clipboard
The Epidemiological Importance of Subclinical Tuberculosis. A Critical Reappraisal
Am J Respir Crit Care Med.
.
No abstract available
Figures
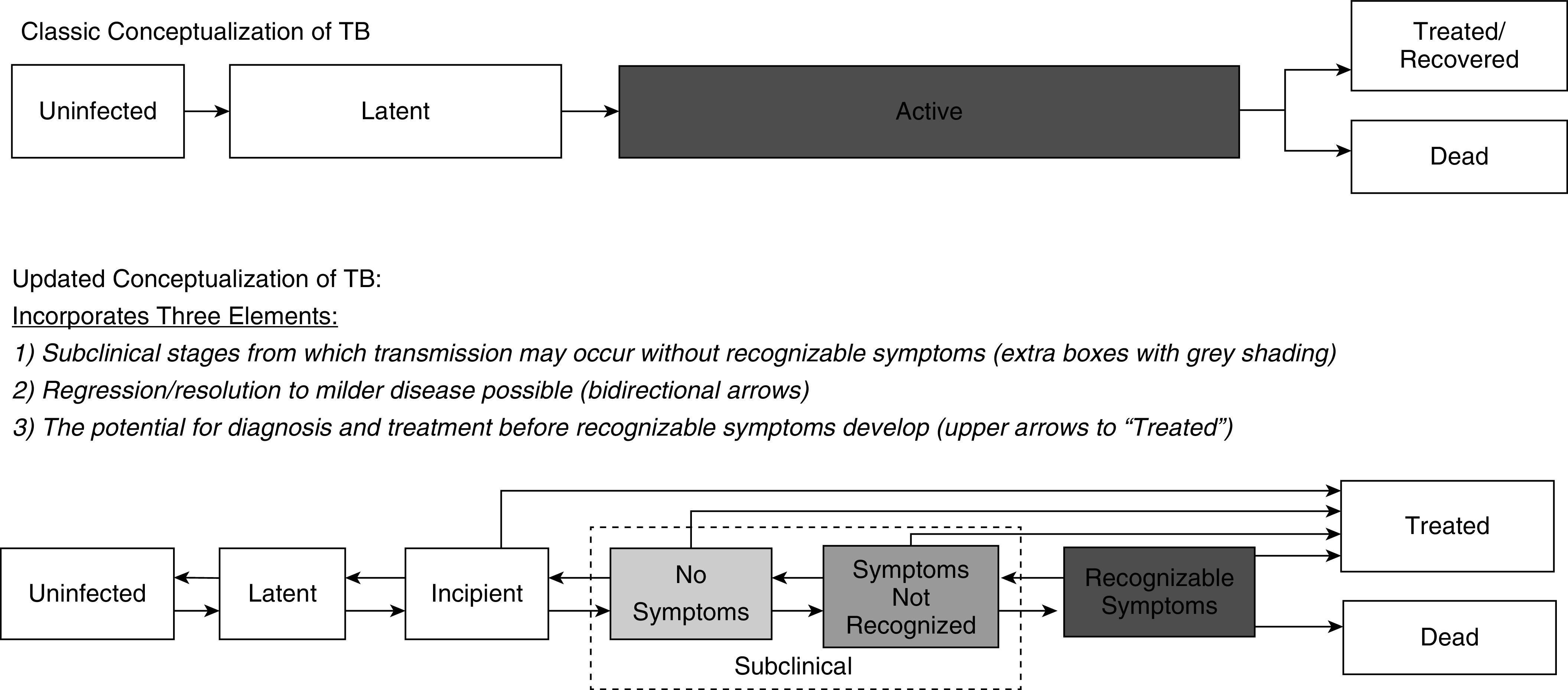
The spectrum of tuberculosis (TB) disease. The top panel shows a “classic” conceptualization of TB as a two-stage entity with inevitable forward progression, transmission (denoted by gray shading) occurring only from those with active TB, and diagnosis and treatment implicitly focused on people with symptomatic (“active”) TB. Others have demonstrated that this conceptualization is an oversimplification, namely, that the development of active TB represents distinct incipient and subclinical stages (5, 6). In the bottom panel, we further expand on this understanding, presenting an updated conceptualization of the spectrum of TB disease, illustrating that individuals with subclinical TB may be truly asymptomatic or have symptoms that are not recognized, both progression and regression across stages occur without inevitable development of recognizable symptoms, and individuals with milder forms of TB disease can be effectively diagnosed and treated. Shading intensity indicates that both subclinical and active TB states may be infectious and that infectiousness is likely to increase with more advanced disease, although the degree of correlation is uncertain.
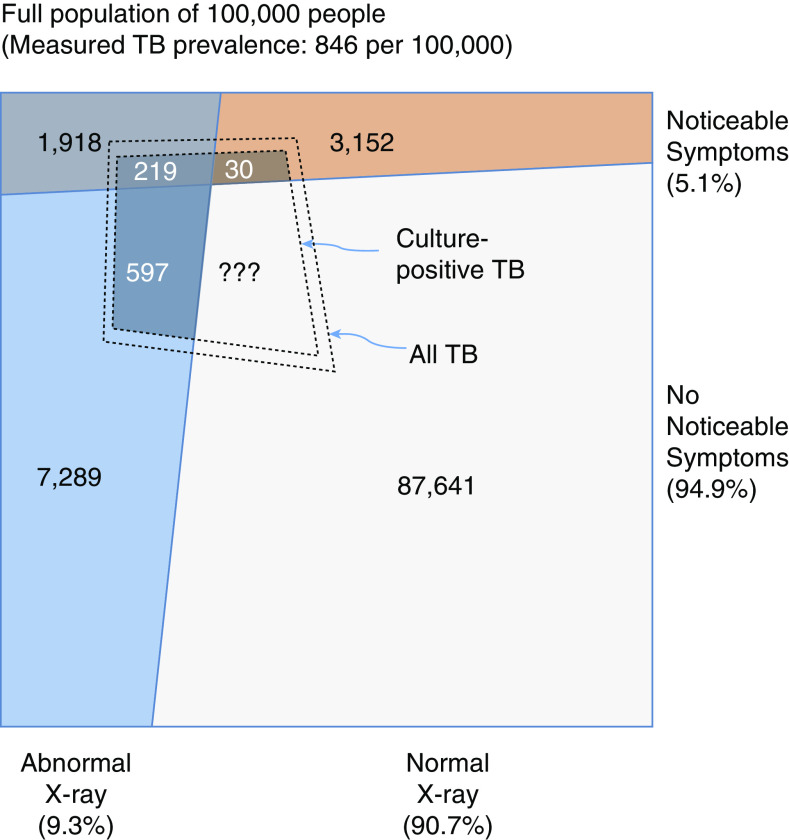
Relationship between symptoms, chest X-ray findings, and culture-confirmed tuberculosis (TB). The outer box represents a population of 100,000, based on the extrapolation of crude results from the 2011 Cambodia National TB Prevalence Survey (55). The inner dashed quadrilateral denotes the number of people with TB detected by sputum culture, and the dashed quadrilateral just outside it indicates all TB disease that would be identified by an optimally sensitive reference standard. In this survey—like in most TB prevalence surveys—only individuals with symptoms or abnormal chest X-ray findings submitted sputum for evaluation. Thus, the TB status of those with normal chest X-ray findings and no reported symptoms is unknown; however, it can be inferred. Specifically, the sensitivity of chest X-ray for symptomatic individuals with culture-positive TB is 219/249 = 88% in this survey. The sensitivity of chest X-ray for culture-positive TB that is asymptomatic would be expected to be lower than for symptomatic TB, but even if it were 88%, this would imply at least 597/0.88 − 597 = 81 individuals with culture-positive TB who would be missed by a combination of chest X-ray and symptom screening. After accounting for correlation between symptoms and X-ray, the likely burden of missed subclinical TB is substantially higher. In other settings and surveys, this burden of radiographically undetectable but culture-positive prevalent TB will vary, and it may be higher in settings of high HIV prevalence.
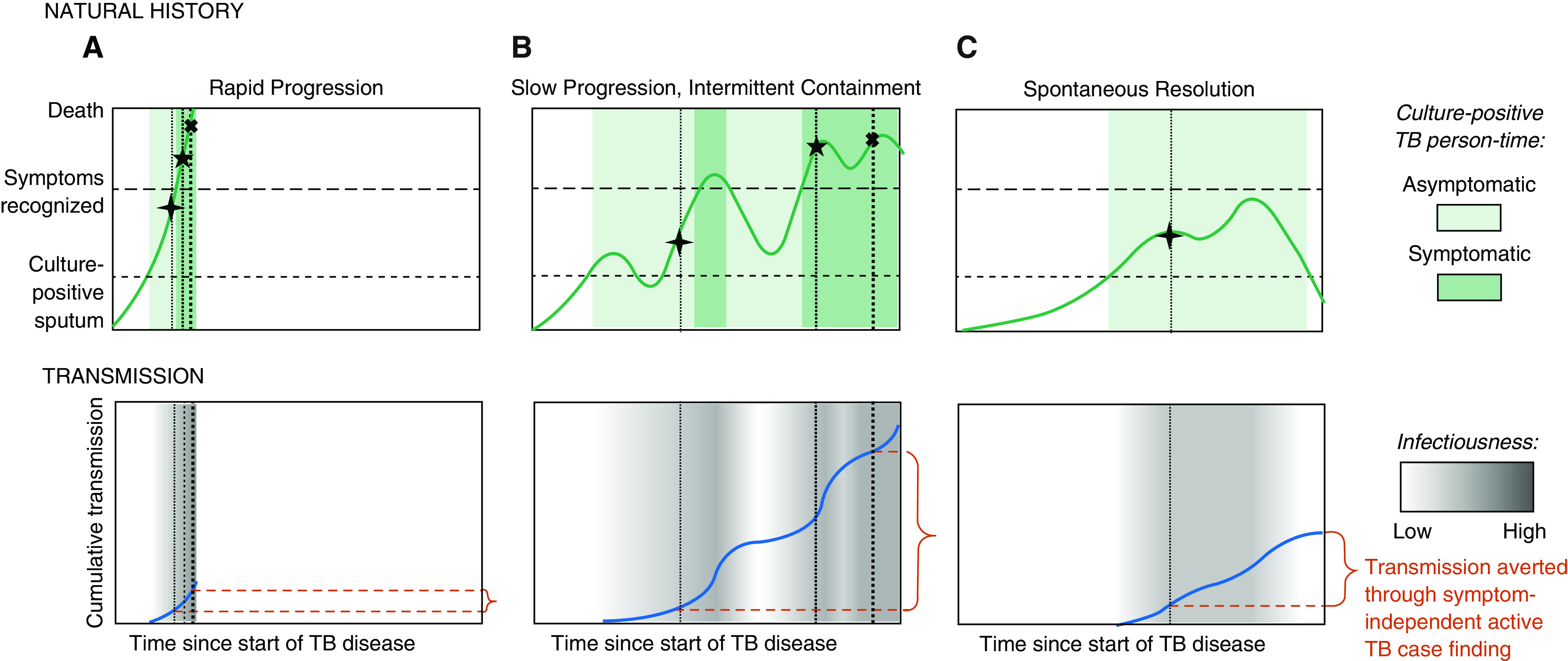
Three paradigmatic patient trajectories of tuberculosis (TB) natural history, transmission, and diagnosis. The top row shows three possible trajectories of TB natural history in the absence of treatment, ordered from the most aggressive (e.g., in those with the weakest immune response) to the most indolent (e.g., those with robust immune responses). The y axis of this top row corresponds with the patient’s burden of disease (abstractly conceptualized), with horizontal lines denoting thresholds above which viable Mycobacterium tuberculosis might be detected in sputum (lower dashed line corresponding with active TB), individuals would confirm TB symptoms if asked during screening (upper dashed line), and death occurs (upper boundary). Note that individuals with TB may have symptoms below the “symptoms recognized” line, but those symptoms (e.g., mild cough) may not be sufficiently recognizable to warrant care seeking or a positive response to a standard symptom screen. Shaded areas denote periods of time during which TB is microbiologically confirmable, with dark shading corresponding with periods of time during which symptoms are recognizable, illustrating that people whose symptoms progress more slowly spend more time in a microbiologically confirmable state. The bottom row presents the amount of M. tuberculosis transmission (in arbitrary units) that might occur during each of these paradigmatic trajectories, with intensity of transmission (per unit person-time) denoted by the darkness of gray shading and cumulative transmission over time denoted by the height of the dark blue line. Vertical dotted lines with corresponding symbols illustrate points of time during which diagnosis might occur, as follows: the first (cross) through active case finding that does not rely on symptom screening, the second (star) through symptom-triggered active case finding, and the third (X) through patient-triggered symptomatic care seeking. The degree to which detecting subclinical cases might avert M. tuberculosis transmission on a population level (shown in red braces) therefore depends on the relative frequency of each trajectory and the shape of each transmission-versus-time curve. A shows rapid progression, B slow progression with intermittent containment, and C spontaneous resolution.
Comment in
-
Subclinical Tuberculosis: Some Flies in the Ointment.Am J Respir Crit Care Med. 2021 May 15;203(10):1327-1328. doi: 10.1164/rccm.202101-0227LE. Am J Respir Crit Care Med. 2021. PMID: 33689597 Free PMC article. No abstract available.
-
Reply to Pierce: Subclinical Tuberculosis: Some Flies in the Ointment.Am J Respir Crit Care Med. 2021 May 15;203(10):1328-1329. doi: 10.1164/rccm.202102-0367LE. Am J Respir Crit Care Med. 2021. PMID: 33689676 Free PMC article. No abstract available.
References
-
- Farley TA, Cohen DA, Elkins W. Asymptomatic sexually transmitted diseases: the case for screening. Prev Med. 2003;36:502–509. - PubMed
-
- Bousema T, Okell L, Felger I, Drakeley C. Asymptomatic malaria infections: detectability, transmissibility and public health relevance. Nat Rev Microbiol. 2014;12:833–840. - PubMed
-
- World Health Organization. Geneva, Switzerland: World Health Organization; 2015. The END TB strategy. [accessed 2020 Jun 15]. Available from: https://www.who.int/tb/End_TB_brochure.pdf?ua=1.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
