

Urinary Sodium and Potassium, and Risk of Ischemic and Hemorrhagic Stroke (INTERSTROKE): A Case-Control Study
- PMID: 33197265
- PMCID: PMC8057138
- DOI: 10.1093/ajh/hpaa176
Urinary Sodium and Potassium, and Risk of Ischemic and Hemorrhagic Stroke (INTERSTROKE): A Case-Control Study
Abstract
Background: Although low sodium intake (<2 g/day) and high potassium intake (>3.5 g/day) are proposed as public health interventions to reduce stroke risk, there is uncertainty about the benefit and feasibility of this combined recommendation on prevention of stroke.
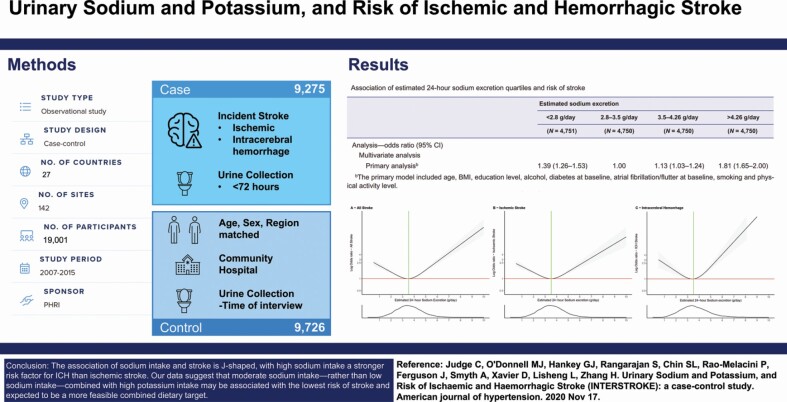
Methods: We obtained random urine samples from 9,275 cases of acute first stroke and 9,726 matched controls from 27 countries and estimated the 24-hour sodium and potassium excretion, a surrogate for intake, using the Tanaka formula. Using multivariable conditional logistic regression, we determined the associations of estimated 24-hour urinary sodium and potassium excretion with stroke and its subtypes.
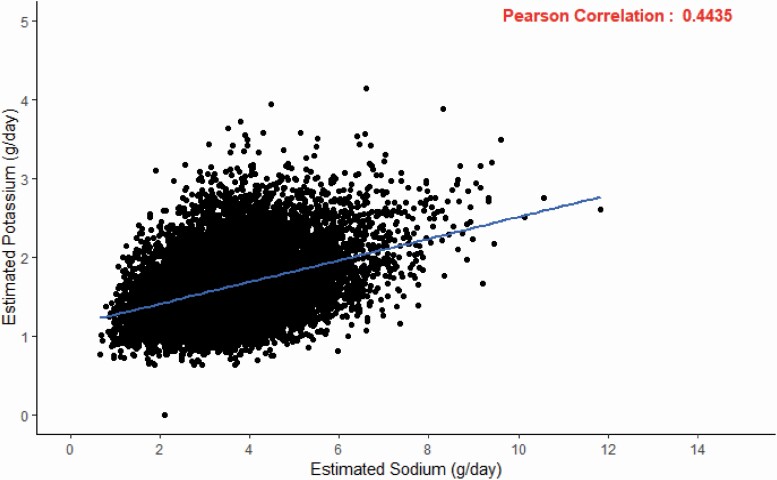
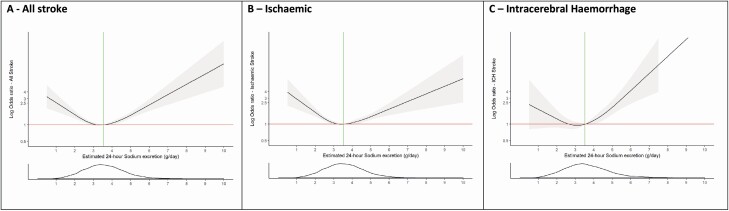
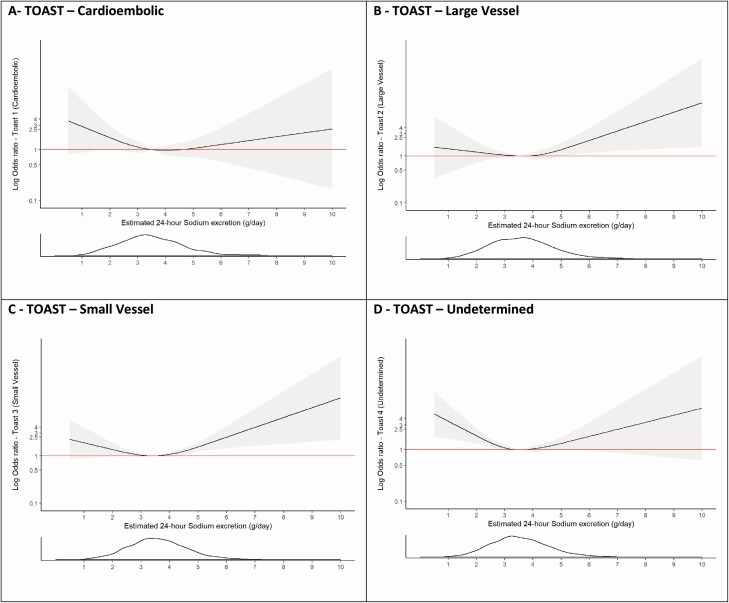
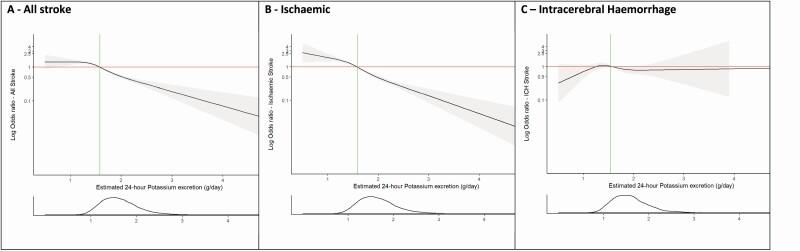
Results: Compared with an estimated urinary sodium excretion of 2.8-3.5 g/day (reference), higher (>4.26 g/day) (odds ratio [OR] 1.81; 95% confidence interval [CI], 1.65-2.00) and lower (<2.8 g/day) sodium excretion (OR 1.39; 95% CI, 1.26-1.53) were significantly associated with increased risk of stroke. The stroke risk associated with the highest quartile of sodium intake (sodium excretion >4.26 g/day) was significantly greater (P < 0.001) for intracerebral hemorrhage (ICH) (OR 2.38; 95% CI, 1.93-2.92) than for ischemic stroke (OR 1.67; 95% CI, 1.50-1.87). Urinary potassium was inversely and linearly associated with risk of stroke, and stronger for ischemic stroke than ICH (P = 0.026). In an analysis of combined sodium and potassium excretion, the combination of high potassium intake (>1.58 g/day) and moderate sodium intake (2.8-3.5 g/day) was associated with the lowest risk of stroke.
Conclusions: The association of sodium intake and stroke is J-shaped, with high sodium intake a stronger risk factor for ICH than ischemic stroke. Our data suggest that moderate sodium intake-rather than low sodium intake-combined with high potassium intake may be associated with the lowest risk of stroke and expected to be a more feasible combined dietary target.
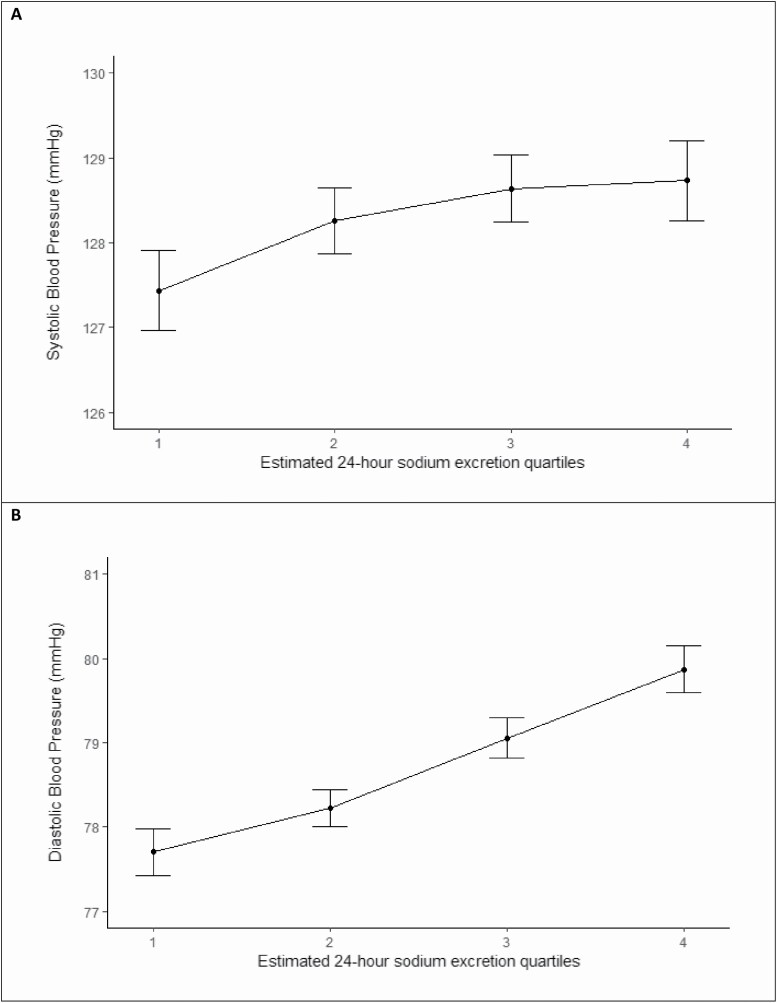
Keywords: blood pressure; hypertension; intracerebral hemorrhage; ischemic stroke; potassium; sodium; stroke.
© The Author(s) 2020. Published by Oxford University Press on behalf of American Journal of Hypertension, Ltd.
Figures
References
-
- O’Donnell MJ, Chin SL, Rangarajan S, Xavier D, Liu L, Zhang H, Rao-Melacini P, Zhang X, Pais P, Agapay S, Lopez-Jaramillo P, Damasceno A, Langhorne P, McQueen MJ, Rosengren A, Dehghan M, Hankey GJ, Dans AL, Elsayed A, Avezum A, Mondo C, Diener HC, Ryglewicz D, Czlonkowska A, Pogosova N, Weimar C, Iqbal R, Diaz R, Yusoff K, Yusufali A, Oguz A, Wang X, Penaherrera E, Lanas F, Ogah OS, Ogunniyi A, Iversen HK, Malaga G, Rumboldt Z, Oveisgharan S, Al Hussain F, Magazi D, Nilanont Y, Ferguson J, Pare G, Yusuf S; INTERSTROKE investigators . Global and regional effects of potentially modifiable risk factors associated with acute stroke in 32 countries (INTERSTROKE): a case-control study. Lancet 2016; 388:761–775. - PubMed
-
- Mente A, O’Donnell MJ, Rangarajan S, McQueen MJ, Poirier P, Wielgosz A, Morrison H, Li W, Wang X, Di C, Mony P, Devanath A, Rosengren A, Oguz A, Zatonska K, Yusufali AH, Lopez-Jaramillo P, Avezum A, Ismail N, Lanas F, Puoane T, Diaz R, Kelishadi R, Iqbal R, Yusuf R, Chifamba J, Khatib R, Teo K, Yusuf S; PURE Investigators . Association of urinary sodium and potassium excretion with blood pressure. N Engl J Med 2014; 371:601–611. - PubMed
-
- World Health Organization (WHO). Guideline: Sodium Intake for Adults and Children [Internet]. Geneva, 2012. [cited 19 November 2018]. http://www.who.int/nutrition/publications/guidelines/sodium_intake_print...
-
- Lloyd-Jones DM, Hong Y, Labarthe D, Mozaffarian D, Appel LJ, Van Horn L, Greenlund K, Daniels S, Nichol G, Tomaselli GF, Arnett DK, Fonarow GC, Ho PM, Lauer MS, Masoudi FA, Robertson RM, Roger V, Schwamm LH, Sorlie P, Yancy CW, Rosamond WD; American Heart Association Strategic Planning Task Force and Statistics Committee . Defining and setting national goals for cardiovascular health promotion and disease reduction: the American Heart Association’s strategic Impact Goal through 2020 and beyond. Circulation 2010; 121:586–613. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
