

Serum Myostatin Predicts the Risk of Hepatocellular Carcinoma in Patients with Alcoholic Cirrhosis: A Multicenter Study
- PMID: 33198216
- PMCID: PMC7697795
- DOI: 10.3390/cancers12113347
Serum Myostatin Predicts the Risk of Hepatocellular Carcinoma in Patients with Alcoholic Cirrhosis: A Multicenter Study
Abstract
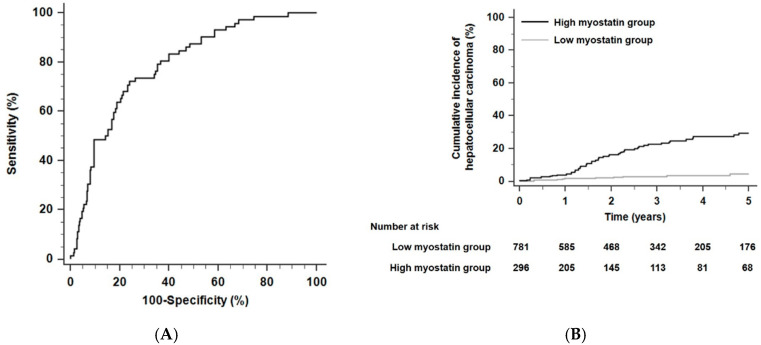
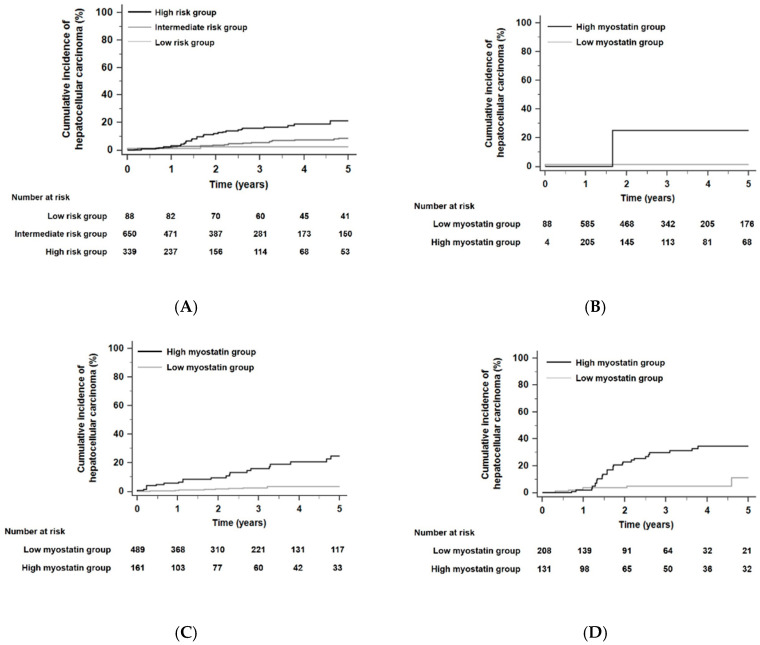
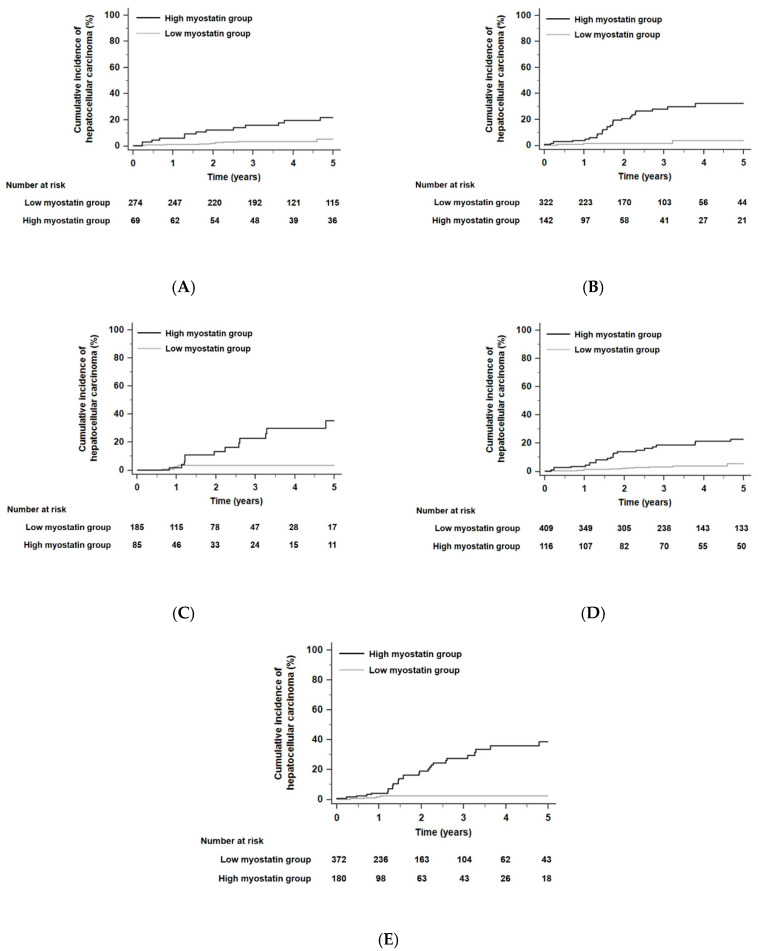
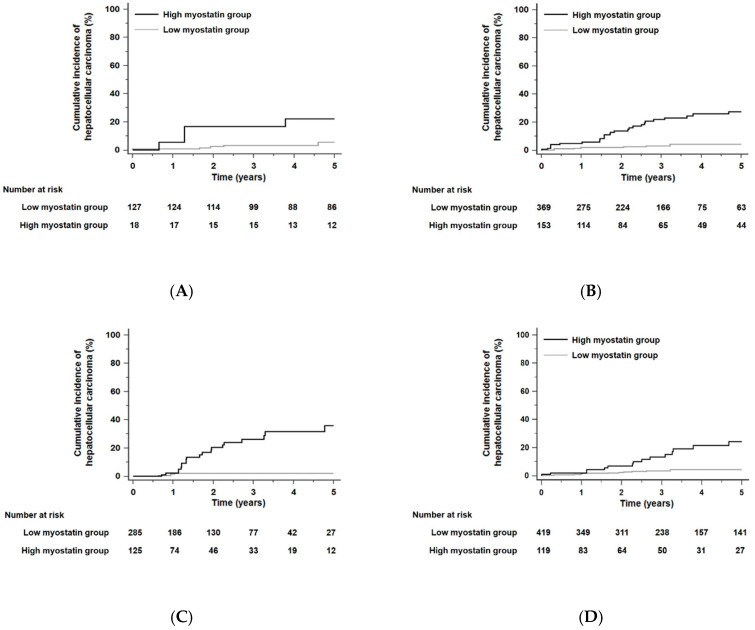
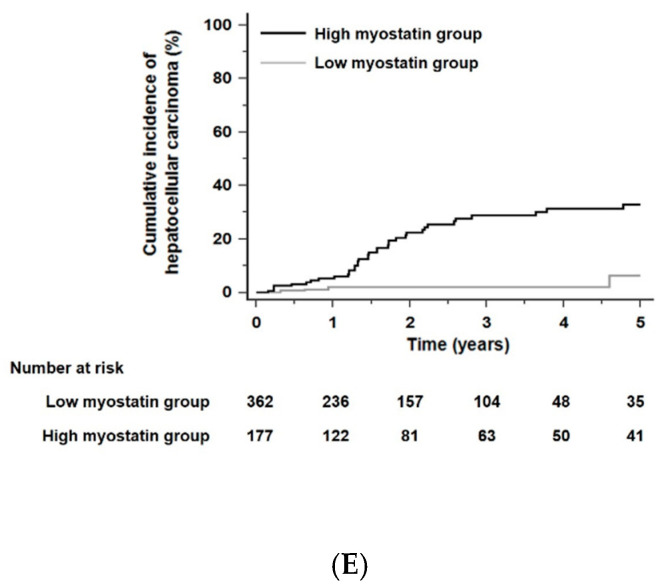
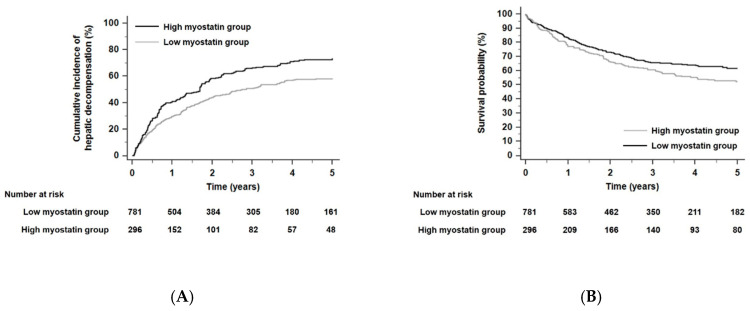
Background and Aim: Previous studies reported that serum myostatin is associated with sarcopenia. We aimed to elucidate the association between serum myostatin levels and hepatocellular carcinoma (HCC) development in patients with alcoholic liver cirrhosis (ALC). Methods: This retrospective, multicenter study assessed 1077 Asian ALC patients enrolled from 2007 to 2017. The primary endpoint was the development of HCC within 5 years. Cox proportional hazards model analyses were used to assess the association of serum myostatin levels and HCC development. The time-dependent areas under the receiver operating characteristic curve (AUROC) of serum myostatin for 5-year HCC development were calculated. Serum myostatin levels were measured using an enzyme-linked immunosorbent assay with samples collected on the index date. Results: During a median follow-up of 2.5 years, 5-year cumulative HCC incidence rates were 6.7% in the total population. The median level of serum myostatin was 3.3 ng/mL (interquartile, 2.1-5.2 ng/mL). The AUROC of serum myostatin for 5-year HCC development was 0.78 (95% confidence interval [CI], 0.76-0.81). In Cox proportional hazards model analyses, age, gender, platelet counts, and serum myostatin levels were independent risk factors for HCC development (adjusted hazard ratios [HRs] of age, male gender, platelet counts, and serum myostatin: 1.03, 2.79, 0.996, 1.18, respectively; all p < 0.05). Patients with high myostatin levels had a significantly higher risk of 5-year HCC development than those with low myostatin levels (HR 7.53, p < 0.001). Conclusion: Higher serum myostatin levels were significantly associated with a higher risk of developing HCC in ALC patients, which could identify high-risk patients who need stringent surveillance.
Keywords: cirrhosis; hepatocellular carcinoma; myostatin.
Conflict of interest statement
These authors disclose no conflicts of interest.
Figures
References
-
- St-Onge M.P. Relationship between body composition changes and changes in physical function and metabolic risk factors in aging. Curr. Opin. Clin. Nutr. Metab. Care. 2005;8:523–528. - PubMed
-
- Gu D.H., Kim M.Y., Seo Y.S., Kim S.G., Lee H.A., Kim T.H., Jung Y.K., Kandemir A., Kim J.H., An H., et al. Clinical usefulness of psoas muscle thickness for the diagnosis of sarcopenia in patients with liver cirrhosis. Clin. Mol. Hepatol. 2018;24:319–330. doi: 10.3350/cmh.2017.0077. - DOI - PMC - PubMed
Grants and funding
- 2017R1D1A1B03031499/Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education
- 2020R1C1C1004112/the National Research Foundation of Korea (NRF) grant funded by the Korea government
- None/the Research Supporting Program of the Korean Association for the Study of the Liver and the Korean Liver Foundation
- None/2020 Kangwon National University Hospital
LinkOut - more resources
Full Text Sources
