

Cost-effectiveness of Artificial Intelligence for Proximal Caries Detection
- PMID: 33198554
- PMCID: PMC7985854
- DOI: 10.1177/0022034520972335
Cost-effectiveness of Artificial Intelligence for Proximal Caries Detection
Abstract
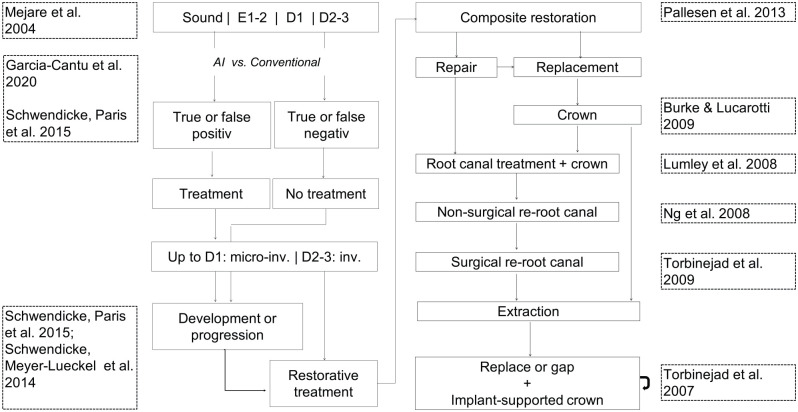
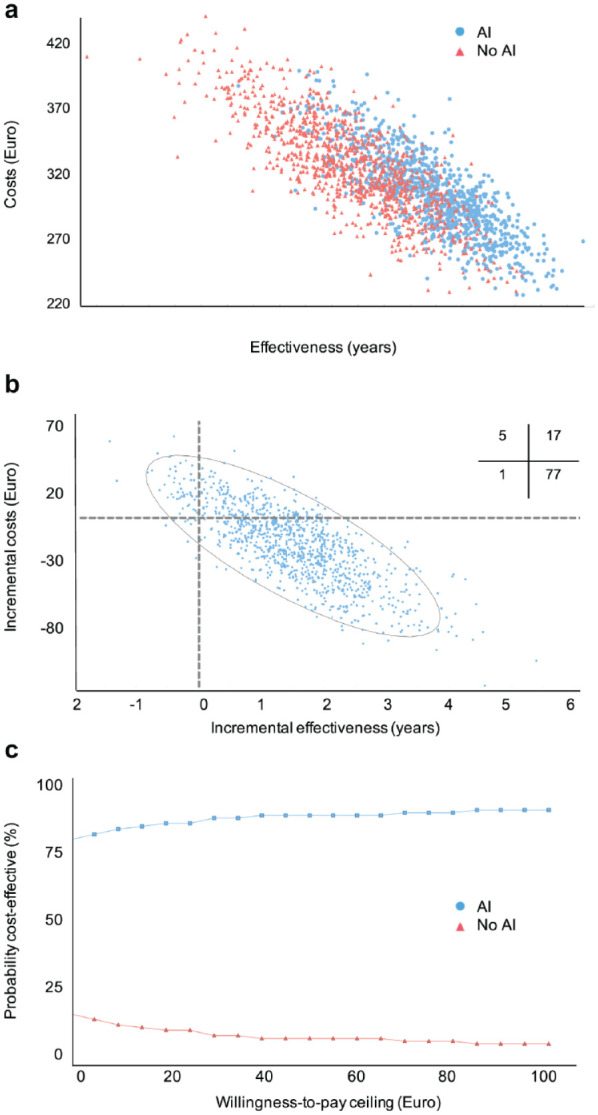
Artificial intelligence (AI) can assist dentists in image assessment, for example, caries detection. The wider health and cost impact of employing AI for dental diagnostics has not yet been evaluated. We compared the cost-effectiveness of proximal caries detection on bitewing radiographs with versus without AI. U-Net, a fully convolutional neural network, had been trained, validated, and tested on 3,293, 252, and 141 bitewing radiographs, respectively, on which 4 experienced dentists had marked carious lesions (reference test). Lesions were stratified for initial lesions (E1/E2/D1, presumed noncavitated, receiving caries infiltration if detected) and advanced lesions (D2/D3, presumed cavitated, receiving restorative care if detected). A Markov model was used to simulate the consequences of true- and false-positive and true- and false-negative detections, as well as the subsequent decisions over the lifetime of patients. A German mixed-payers perspective was adopted. Our health outcome was tooth retention years. Costs were measured in 2020 euro. Monte-Carlo microsimulations and univariate and probabilistic sensitivity analyses were conducted. The incremental cost-effectiveness ratio (ICER) and the cost-effectiveness acceptability at different willingness-to-pay thresholds were quantified. AI showed an accuracy of 0.80; dentists' mean accuracy was significantly lower at 0.71 (minimum-maximum: 0.61-0.78, P < 0.05). AI was significantly more sensitive than dentists (0.75 vs. 0.36 [0.19-0.65]; P = 0.006), while its specificity was not significantly lower (0.83 vs. 0.91 [0.69-0.98]; P > 0.05). In the base-case scenario, AI was more effective (tooth retention for a mean 64 [2.5%-97.5%: 61-65] y) and less costly (298 [244-367] euro) than assessment without AI (62 [59-64] y; 322 [257-394] euro). The ICER was -13.9 euro/y (i.e., AI saved money at higher effectiveness). In the majority (>77%) of all cases, AI was less costly and more effective. Applying AI for caries detection is likely to be cost-effective, mainly as fewer lesions remain undetected. Notably, this cost-effectiveness requires dentists to manage detected early lesions nonrestoratively.
Keywords: caries diagnosis/prevention; computer simulation; decision making; dental; economic evaluation; radiology.
Conflict of interest statement
Figures
References
-
- Baelum V, Hintze H, Wenzel A, Danielsen B, Nyvad B. 2012. Implications of caries diagnostic strategies for clinical management decisions. Community Dent Oral Epidemiol. 40(3):257–266. - PubMed
-
- Briggs AH, O’Brien BJ, Blackhouse G. 2002. Thinking outside the box: recent advances in the analysis and presentation of uncertainty in cost-effectiveness studies. Annu Rev Public Health. 23(1):377–401. - PubMed
-
- Burke FJT, Lucarotti PSK. 2009. Ten-year outcome of crowns placed within the General Dental Services in England and Wales. J Dent. 37(1):12–24. - PubMed
-
- Ferrari M, Vichi A, Fadda GM, Cagidiaco MC, Tay FR, Breschi L, Polimeni A, Goracci C. 2012. A randomized controlled trial of endodontically treated and restored premolars. J Dent Res. 91(7 suppl):S72–S78. - PubMed
-
- Frencken JE, Innes NP, Schwendicke F. 2016. Managing carious lesions: why do we need consensus on terminology and clinical recommendations on carious tissue removal? Adv Dent Res. 28(2):46–48. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
